
2 Theories of Aging
Theories of Aging
We are slowly isolating the genes involved
with the aging process. We do not have the
fountain of youth, but I think, in the coming
decades, we will unravel the aging process
at the genetic level.– Michio Kaku

Aging is the process of getting older and a reflection of all the changes that occur over a lifetime. Aging includes both growth and development. To the young, getting older is exciting because it leads to greater independence. To those in middle or late adulthood age is associated with physical decline, regardless of how athletically fit or healthy one might be.
The human lifespan is frequently divided into age related periods however, there is no firm rule about the specific ages and how they should be characterized. Figure 2.1. provides just one example of periods of development based on years of age. The prenatal period, which begins at the time of conception and continues until birth, is delineated by weeks of gestation. The first 2 weeks after conception are referred to as the germinal period. The embryonic period falls between weeks 2-8, followed by the fetal period of weeks 9-38.
Based on research in recent years, some scientists have suggested that the adolescence period in table in Figure 2.1 may need to be modified. Studies of adolescent and young adult brains show a remarkable increase in brain synapses during this period and beyond, perhaps indicating that the period of adolescence may actually continue until age 24
(Sawyer, et al, 2018).

Figure 2.1 Periods of Development
Gerontologists and others have observed that the late adulthood period is not descriptive enough to capture the differences between 65 year olds and 85 year old and have suggested the sub-categories of young-old for 65-74 years of age and middle-old for 75-84 years of age. The last category, from 85 years of age to death, is referred to as the oldest-old (Lee, et al, 2018).
The study of normal aging has helped scientists across many disciplines to understand what it means to grow old. Although people age differently, there are certain common changes that are experienced by everyone. Hearing and vision, for example, have been observed to decline through middle and late adulthood, even when no known pathological process can be identified. On the other hand, observations of older adults having arthritis and diabetes are due to pathology rather than the normal aging process.
Theories of Aging
Many theories have been proposed to answer the question, “How do we age?” Generally, the theories fall into 2 categories. Programmed theories are those that promote a biological timetable that is regulated by gene expression. Damage or error theories suggest that environmental insults result in expanding damage at various levels of the organism. This chapter includes just a few examples of theories that fall into either the programmed or damage categories.
Hayflick Limit Theory
Leonard Hayflick (1928- ) and his colleague Paul Moorhead discovered that many human cells have a limited capacity to reproduce themselves. From cultured studies of fetal and embryonic tissue, they observed that cells can undergo only 40-60 cell divisions and then cell division ceases. This number is often referred to as the Hayflick Limit (Hayflick, 1996). Some scientists have expanded the idea of cellular division as an explanation of aging into what is known as the replicative senescence hypothesis of aging. They propose that what determines the limit for dividing cells is the length of the cells’ telomeres because each time a cell divides, it must double its chromosomes. However, each time a chromosome reproduces itself, it loses a small bit of its telomeres. After 40-60 doublings, the cells have shortened telomeres, which allow them to live, but they can no longer divide.

Figure 2.2 Telomere shortening
It does not appear however, that shortened telomeres are the complete explanation for the aging process. Not all types of tissue contain replicating cells and telomere shortening is not universal among species. In addition, the role the enzyme telomerase plays in telomere length, cell reproduction and cancer is complex, requiring much greater understanding before conclusions can be drawn about the effect cell replication and telomere length plays in normal aging (Shammas, 2011).
Neuroendocrine Theory
The neuroendocrine system includes complex connections between the brain, nervous system and the endocrine glands, which produce hormones. Vladimir Dilman (1925-1994) and Ward Dean claimed that aging is a direct result of age-related changes in the neuroendocrine system. Over time, 2 very important structures of the endocrine system, the hypothalamus and the pituitary, become less functional, which can negatively effect of proper release of hormones from other organs and glands. In addition, receptors within the neuroendocrine system become compromised, leading to a decreased sensitivity of circulating levels of hormones which can further interfere with neuroendocrine regulation. Because hormones have wide reaching effects on every system in the body and play important roles in vital functions such as blood pressure regulation, metabolism, growth and sexual functioning, failure of the neuroendocrine system to functional properly will lead to failure of multiple bodily systems.
Cross-Linkage Theory
In 1942, Johan Bjorksten (1907-1995) conceived the Cross-Linkage Theory of Aging, which is now frequently referred to as the Glycosylation Theory of Aging. Bjorksten proposed that during the aging process, proteins, DNA and other molecules develop non-functional attachments to each other known as cross-links (Bjorksten, 1968). These cross-linked proteins and molecules experience decreased mobility which results in damaged cells and tissues, thereby slowing down bodily processes, resulting in aging.
One of the main ways cross-linkage occurs is through the process of glycosylation in which glucose molecules stick to proteins, thereby transforming them into advanced glycosylation end products (AGEs). When the sticky ends of the AGEs adhere to the nearby proteins, they form a permanent cross-linkage that interferes with the proteins’ ability to function. Cross-linkages have been associated with integumentary changes noted with aging as well as cataracts and atherosclerosis. Recent studies have demonstrated that glycosylation contributes to the formation of beta-amyloid, a protein associated with Alzheimer’s disease (Knight, 1995).
Free Radical Theory
The Free Radical Theory, also known as the Oxidative Damage Hypothesis was proposed by Denham Harman (1916-2014) in 1956. Oxidative free radicals or reactive oxygen species (ROS), occur as a toxic byproduct of normal cell metabolism. Substances known a antioxidants pair up with the free radicals and neutralize their potential damage. However, when free radicals are unable to be linked with antioxidants, they cause oxidative damage to DNA, proteins and mitochondria. The accumulation of damage is a direct cause of aging (Harman, 1992). Formation of free radicals can be a result of environmental factors such as radiation and air pollution, and lifestyle such as poor dietary choices and smoking. Proponents of the free radical therapy also claim that oxidative damage is associated with cross-linkages of proteins and formation of age pigments, contributing to age-related pathologies including heart disease, Alzheimer’s, cancer and diabetes.
The study of aging continues in an effort to explain how we age. In all likelihood, a number of theories and hypothesis about the aging process may be true. Identification of mechanisms that affect aging will hopefully lead to interventions and recommendations for lifestyle decisions that will promote longer and healthier lives.
Life Expectancy
The rate and progression of the aging process can vary greatly from one individual to the next. However over time, aging affects the cells of every major organ of the body and eventually the organism dies. Lifespan simply stated, is the length of life. The application of Hayflick’s Limit Theory would predict that maximal lifespan is approximately 115 years. Jeanne Calment, exceeded that prediction by 7 years and died at 122 years of age. The oldest man, Jiroemon Kimura died in Japan at the age of 116. Figure 2.4 illustrates life expectancies across the world and is likely representative of the influence genetics and environment play on lifespan. In 2021, the life expectancy was United States was 78.99 years. Women fared better than men, with a life expectancy of 81.1 years compared to 76.1 years for me.
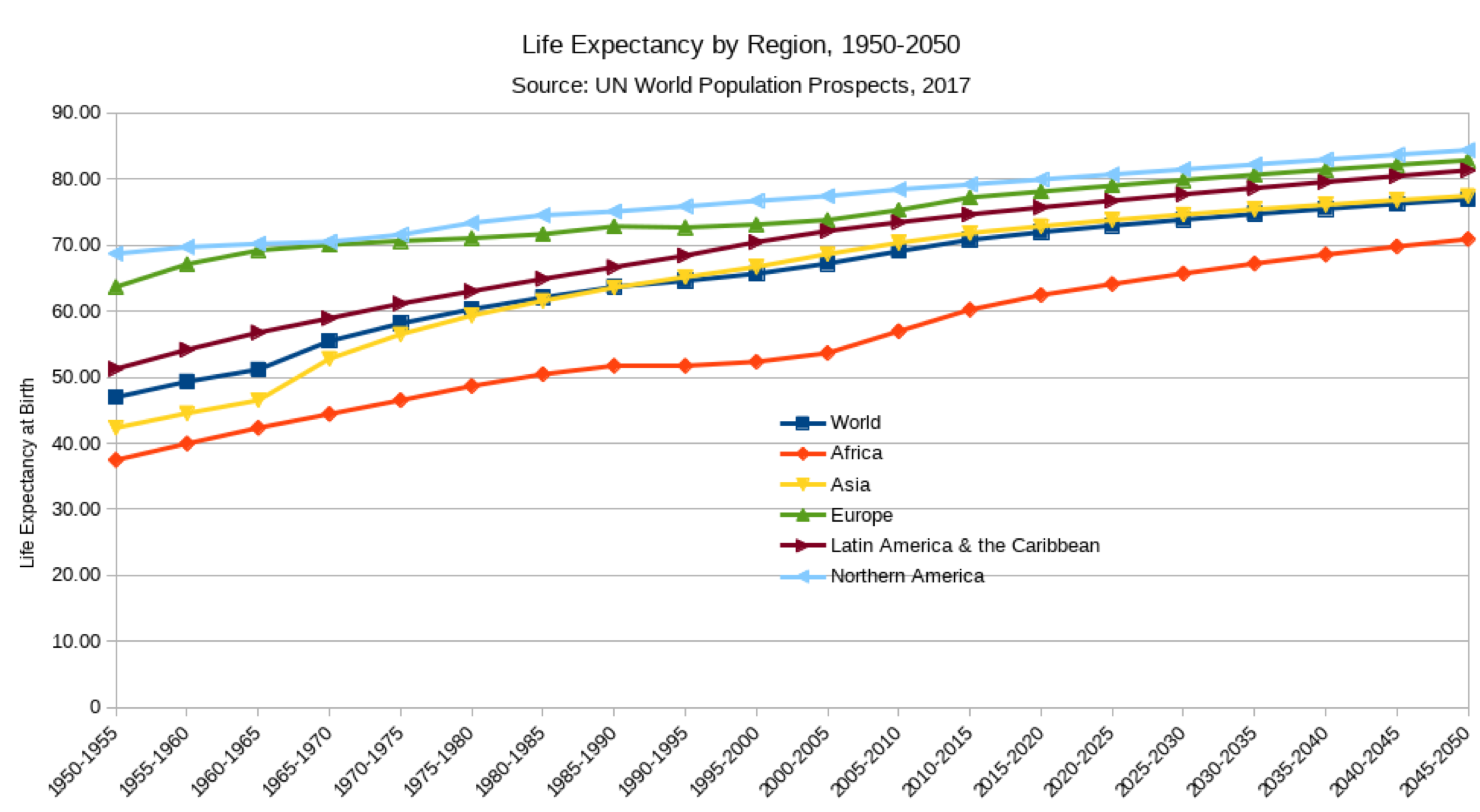
2.4 Global Life Expectation
Death and Dying
Death is a certainty of life. For some death will occur suddenly, most commonly due to cardiac arrest. Others will die of traumatic injuries, either within minutes, hours, or even weeks after the injury. The vast majority of people however, die from disease or natural causes. In 2020, the leading cause for death in the United States was heart disease, followed by
cancer. For the first time in history, the third leading cause of death in the United State was COVID-19. In the distant fourth and fifth positions are unintentional injuries and stroke, followed by chronic lower respiratory disease (Ahmed & Anderson, 2021).
Regardless of the mechanism of death, the Uniform Determination of Death Act (UDDA), which has been adopted nationwide, provides 2 definitions for when a person may be legally declared dead: 1) irreversible cessation of circulatory and respiratory functions, or 2) irreversible cessation of all function of the entire brain, including the brain stem.
XXXXXXXXXXXXXXXXXXX
The most common type of death is due to cessation of circulatory and respiratory functions. Sometimes however, as in the second definition, a person may be kept “alive” through the use of technology, even though there is no brain activity. Most states consider brain dead individuals legally dead and remove them from life support, even though the body’s other life functions may be maintained to support organ donation.
For over 90% of individuals, death will occur after a long period of illness with gradual deterioration until the active dying phase at the end. The last hours of life may be some of the most significant because they provide the last opportunity to finish business, create final memories, find peace and say goodbyes.
Physiologic changes that occur during the active dying phase include nearly every system of the body. Most people lose their appetite and reduce food intake long before they reach their final hours of life. In addition, it should be anticipated that many people will reduce their fluid intake or stop drinking entirely, long before they die. Although some families may view this “giving up”, it is important to realize that loss of appetite and a reduction of fluid intake is normal at this stage and may in fact, be beneficial during the process of dying.
As cardiac output and intravascular volume decreases toward the end of life, there will be diminished peripheral blood perfusion. Conditions such as tachycardia, hypertension and observations including the pooling of venous blood and mottling of the skin are normal. Kidney perfusion diminishes and urine output is negligible or absent. Weakness and fatigue increase as people get closer to death. In the last few hours of life it is unlikely that individuals will be able to move around in bed at all.

Figure 2.6 The 2 Roads to Death
The neurologic changes associated with dying tend to present in two different patterns, sometimes described as the two roads to death (Figure 2.6). Most people follow the “usual road”, which includes a decreasing level consciousness and drowsiness. During this time, it may be distressing to friends and family members that the dying person has difficulty communicating. While it is uncertain what unconscious people can hear, observations suggest that awareness may be greater than the ability to respond.
The “difficult road”, travelled by the minority of individuals, includes agitation and delirium due to central nervous system excitation, with or without myoclonic jerks that leads to coma and death. Although this path may be upsetting to family and friends, they should be assured that the process is natural and that what the person is actually experiencing may be very different from what they observe.
Regardless of the path, changes in the dying person’s breathing pattern are indicative of significant neurological compromise. Breaths may become very shallow, and periods of
apnea may occur. Families should be made aware that during this period, the individual is not experiencing a sensation of “suffocation” and that changes in breathing are anticipated during the final stages of the dying.
During the last few hours of life, further decline of neurologic function and weakness will impair an individual’s ability to
swallow, leading to a build up of secretions that are sometimes realized as gurgling or crackling and referred to as the “death rattle”. Also as a result of weakness and neurologic function, individuals may experience incontinence of stool and/or urine during the last few hours of life. Although this is distressing to family members, attention to cleaning and skin care will help the dying individual remain comfortable.
While many fear that pain will increase as a person dies, there is no evidence to support this. Nevertheless, persons in pain during the dying process may benefit from appropriately prescribed opioids. However, it is important not to misread restlessness, agitation, and moaning as signs of pain, as these observations are consistent with terminal delirium. It is important for families to understand the difference between the two and for health care providers to act in the dying person’s best interest.
End of Life Care
When death is a certainty, health care professionals and families will begin to discuss palliative care, which focuses not on life extension, but on the quality of life. According to the World Health Organization,
“Palliative care is an approach that improves the
quality of life of patients and their families facing the
problems associated with life-threatening illness,
through the prevention and relief of suffering by
means of early identification and impeccable assessment and treatment of pain and other problems,
physical, psychosocial and spiritual.”
Goals for end of life care fall into the domains of comfort measures, psychological and spiritual support, and communication with family and others. Under the domain of comfort measures, health care providers with input from the patient, make decisions about symptom management including medications, durable medical equipment and other interventions so that the patient is as free from discomfort as possible. At the same time it is important for the patient to be able to participate in activities of daily living and desirable social activities. Heath care providers also play an important role in describing what to expect during the end of life process and for providing explanations for all possible treatment options. Psychological and spiritual support may come from a variety of individuals and take different forms. The goals are to help the patient process and perhaps make decisions about treatment and care options, as well as assist the patient in dealing with psychological issues such as depression and anxiety. Counselors and spiritual advisors can help patients talk about what it means to die and offer opportunities for the patient to reflect on his or her life. They can also facilitate patient communication with family and others in ways that will ensure that the patient’s desires and wishes are carried out in the most sensitive and appropriate ways.
Final Thoughts
“How can the dead be truly dead when they still live
in the souls of those who are left behind?”
—Carson McCullers, The Heart Is a Lonely Hunter
“Life asked death, ‘Why do people love me but hate
you?’ Death responded, ‘Because you are a beautiful lie and I am a painful truth.”
—Author unknown
References
Ahmad, F.B., & Anderson, R.N. (2021). The leading causes of death in the US for 2020. JAMA 325(18),1829–1830.
Bjorsten, J. (1968). The crosslinage theory of aging. Journal of the American Geriatrics Society, 16(4), 408-427.
Dilman, V. & Dean, W. (1992). The neuroendocrine theory of aging and degenerative disease. Pensacola, FL: Center for Bio-Gerontology.
Harman, D. (1992). Free radical theory of aging. Mutation Research, 275(3-6), 257-266. Hayflick, L. How and Why We Age. New York: Ballantine Books, 1996.
Knight, J.A. (1995). The process and theories of aging. Ann Clin Lab Sci 25(1), 1-12.
Lee, S. B., Oh, J. H., Park, J. H., Choi, S. P., & Wee, J. H. (2018). Differences in youngest-old, middle-old, and oldestold patients who visit the emergency department. Clinical
and Experimental Emergency Medicine, 5(4), 249–255.
Medscape (April, 2018). The last hours of living: practical advice for clinicians: physiologic changes and symptom management. Retreived, April 27, 2018 at https://www.medscape.org/viewarticle/716874_3
Murray, S.A. et al. (2005). Illness trajectories and palliative care. BMJ, 330(7498), 1007-1011.
Sawyer, S.M., et al. (2018). The age of adolescence. The Lancet Child & Adolescent Health, 2(3), 223-228.
Shammas, M.A. (2011). Telomeres, lifestyle, cancer and aging. Current Opinion in Clinical Nutrition and Metabolic Care,
14(1), 28-34.
Images
Title page Theories of Aging [Image File] Retrieved from https://pixabay.com/en/smartphone-face-man-oldbaby-1790833/
Figure 2.1 Periods of Development [Image File] Retrieved from https://classconnection.s3.amazonaws.com/355/flashcards/644355/jpg/intro_to_lifespan1314458203187.jpg
Figure 2.2 Telomere Shortening [Image File] Retrieved from http://sphweb.bumc.bu.edu/otlt/mph-modules/ph/aging/ paste_image2.jpg
Figure. 2.3 Causes of Free Radical Formation [Image File] Retrieved from https://ivao.com/upload/pictures/aging/New_aging/svobodorad4.jpg
Figure 2.4 Global Life Expectancies [Image File] Retrieved
from https://commons.wikimedia.org/wiki/File:Life_Expectancy_At_Birth_By_Region.png
Figure 2.5 Leading Causes of Death for All Ages in the US [Image File] Retrieved from https://images.angelpub.com/2016/25/38516/leadingdeathcauses.jpg
Figure 2.6 The 2 Roads to Death, Originally published in: Freemon FR. Delirium and organic psychosis. In: Organic Mental Disease. Jamaica, NY: SP Medical and Scientific Books; 1981:81-94.
