
8 Cognitive Development & Changes Across the Lifespan
“When looking at the brain, it is important to
go beyond its structure to its function. This
is because often in cognitive disorders, the
structure of the brain is intact, but its function is compromised”.
– Aditi Shankardass

Courtesy of Pacific Northwest National Laboratory
Cognitive functioning includes mental processes such as attention, formation of knowledge, memory, verbal fluency, reasoning, judgement, problem solving, computation, and decision making.
Simply stated, cognition is the process of knowing. Knowledge is the information a person knows, and can be defined as 3 types: 1) declarative knowledge, 2) procedural knowledge, and 3) strategic knowledge (Chi & Ohlsson, 2005). Declarative knowledge is simply knowing factual information. Procedural knowledge is knowing how to do something in accordance with specific rules. Strategic knowledge is knowing the general rules or strategies that apply to many topics. Intelligence is the ability to acquire, understand, retain and apply knowledge to solve problems and enhance performance.
Cognitive development requires at minimum, the processes of attention and memory, both of which begin during infancy and continue to improve through childhood and adolescence, often associated with myelination and glucose uptake activity in the developing brain. The theoretical foundation for how we think about cognitive development was described by Jean Piaget. He proposed that cognitive development occurs in discrete, yet interconnected stages from birth through early adolescence (refer to Chapter 1 for more information about Piaget’s Stages of Cognitive Development).
Verbal Language
During infancy and childhood cognition is often reflected in the development of verbal language. Although there are many instances of very intelligent people who did not speak well until the age of three or four years, most children exhibit at least the desire to verbally communicate with others by the end of the first year.
Pre-speech sounds include cooing, babbling, squealing, grunting and lalling, all of which are produced by repeated movement of the tongue. Some of these sounds can be heard as early as two-three months. By nine months of age, infants will have made every basic sound of the human language and efforts will be made to articulate based on imitation. Family and caregivers should be encouraged to talk and read to infants to allow ample opportunities for imitation. In addition, it’s important to react positively to vocalizations because this will reinforce the behavior and facilitate verbal communication (Oates & Grayson, 2004).
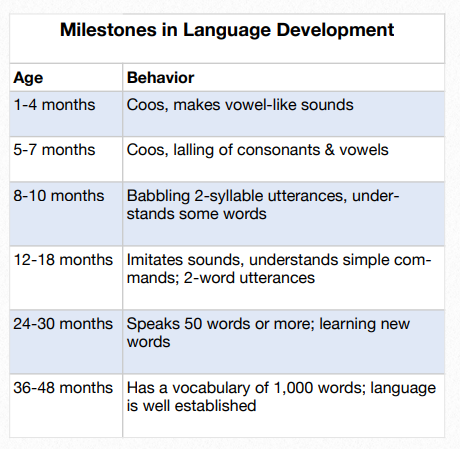
Figure 8.1 Milestones of Language Development
Between the ages of 10-18 months most infants will have spoken their first word, with the average age of approximately 12 months. During this period of time, it is possible for the infant to have a vocabulary of about 6 words. From 1.5 – two years, toddlers will likely be putting two words together, such as “me up” and by three years of age, most will be speaking in phrases or short sentences (Figure 8.1). It is worth noting that at this age, many toddlers will only know one word for an object. For example, young children may know the word “couch” as a
place where mom and dad read stories, but they will not know that it can also be called a “sofa”.
As children prepare for preschool and kindergarten language becomes less egocentric and they are able to engage in various forms of conversations. They have fairly well developed memories for daily events and can talk about those experiences with quite a bit of detail. Figure 8.2 provides some examples of how preschoolers combine language with developing cognitive concepts.
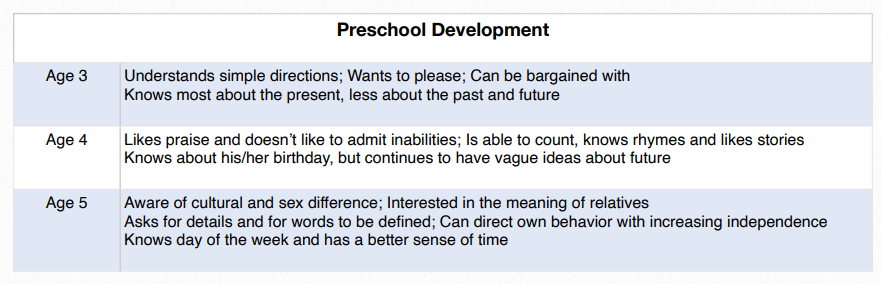
Figure 8.2 Preschool Language and Cognitive Concepts Combined
Cognitive Concepts and Intelligence
Childhood
When young children delay communication through verbal language, cognitive development can be assessed by observing their engagement and interaction with people and the environment. Young children, especially toddlers, learn through activities driven by imitation, exploration and experimentation. Through intrinsic and/or extrinsic reinforcement of these activities, children learn concepts such as object permanence (12-18 months), prediction, problem solving (18-24 months) and symbolic play (2+ years).
Cognitive concepts come about by giving precepts such as events, things, and experiences, a meaningful label. The label implies similarity to some other things, whereas different labels imply that certain things or experiences are different from each other. Concept formation develops with advancement of perceptual processing. Initially, this allows toddlers to realize that dogs can be many different shapes and sizes, and even though they walk on 4 legs and like to be petted, they are not cats. Advances in concept formation include the concepts of relationships such as time, space, number and causation, which may initially be based on immediately observable properties, but eventual are applied in the abstract. At approximately six-seven years of age, children begin to demonstrate the ability to reason in a systematic way about tangible or familiar situations. This allows them to analyze relationships and structure
the environment into meaningful categories (Oates & Grayson, 2004).
There are several cognitive abilities that develop and become refined between the ages of 6-12. The first is classification, which affords children the ability to sort objects according to specific and multiple attributes such as length, size, shape, etc. Seriation is the ability to order objects according to a decreasing or increasing measure.
For example, a child will be able to know that he is taller than his little brother, and shorter than his older sister. Nesting is demonstrated when a child knows how a sub-concept fits into a larger concept. This is demonstrated when a child knows that a race car and a station wagon are different, but are both cars.

8.3 Child Applying Cognitive Concepts While Building
Conservation is the ability to understand that transformation does not alter mass or quality even if there is a change in shape or position. One example is when a ball of clay is formed into different shapes. Regardless of whether the clay is molded to a bird or a ship, it can still be remolded to the original ball without removing or adding clay. Another example is water, which can be frozen or turned into vapor, but it is still the same amount of water. Decentering is the coordination of 2 or more dimensions and the ability to focus on several characteristic simultaneously. Consider a row of 6 blocks spread out that they occupy 8 inches of space compared to 6 blocks that occupy 12 inches of space. The concept of decentering allows an individual to realize that there a not more blocks, they have simply been placed further apart.
Adolescence
Adolescence is a time when the mind has great ability to acquire and use knowledge. It is also the developmental period in which teenagers and even individuals in their early 20s are thinking about and creating a workable philosophy of life. This is a task that requires much abstract and analytic thinking, including inductive and deductive reasoning.
Adolescents use available information to combine ideas into concepts and concepts into constructs. This allows for the development of theories and what Piaget referred to as hypothetic-deductive reasoning, which is the ability to generate hypotheses and systematically test them. This process can lead to the gathering of additional facts and the development of alternate solutions to problems. If not stifled by authorities who promote attention to rigid rules, principles and processes, adolescents can demonstrate highly imaginative thinking which can develop into significant contributions to science, art and music. During adolescence, individuals are developing the capacity to use scientific reasoning and solve hypothetical problems, and are able to work with knowledge of the past and present to inform the future (Steinberg, 2005).
Adulthood
Adults are thought to conceptualize problems and reason with issues differently from adolescents because adults tend to shift from relying solely on logic to combining logic and “common sense”. Admittedly, this may sometimes interfere with developing widely creative ways of solving problems and innovation. Nevertheless, adults tend to face real-world
challenges with a broad spectrum of variables that extend far beyond the awareness of most adolescents. Adults for example, are more likely than adolescents to engage in reasoning that acknowledges that, 1) “truth” may be relative given the context of a situation, 2) all environments have the potential to be unstable, and 3) human behavior is often unpredictable.
Some researchers have conceptualized cognitive development as intelligence. The most widely accepted theory of intelligence is the Cattell-HornCarroll (CHC) Model, an integration of two previously developed theories. The first theory by Cattle and Horn was known as the Gf-Gc model. This was based on the several factors including, but not limited to comprehension knowledge (Gc) also referred to as “crystallized intelligence” and “fluid intelligence (Gf). Crystallized intelligence is defined as the accumulation of knowledge and skills. It reflects
general, procedural and declarative knowledge within a cultural context. Fluid intelligence is the ability to process information and employ novel problem solving strategies that are not dependent on previously learned information (Cattell, 1963).
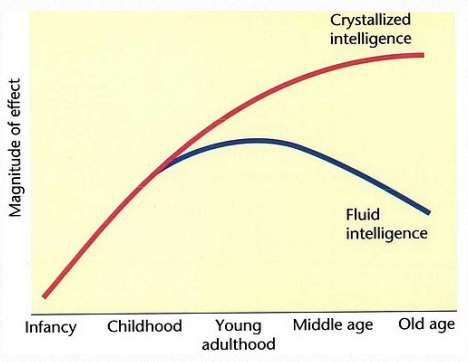
Figure 8.4 Fluid and Crystallized Intelligence Across the Lifespan
The second theory of the CHC model is Raymond B. Carroll’s Three-Stratum theory, a 3-level hierarchical theory that categorized levels of cognition into narrow, broad and general abilities. It was the overlap of elements considered to be a part of intelligence, and discussions between the theorists that brought the Gf-Gc model and the three-stratum theory together to form the CHC model. Factors such as memory, the use of language, and visual and auditory processing, along with fluid and crystallized intelligence, all contribute to overall intelligence.
Capabilities developed during adolescence such as logical and inferential reasoning, concept formation, and hypothesis generation and testing provide the underpinnings of fluid intelligence. Although crystallized and fluid intelligence are different, there is an interaction. Some degree of crystallized intelligence is necessary for fluid intelligence to exist, yet fluid
intelligence plays a role in determining the speed in which crystallized knowledge is accumulated. Crystallized intelligence does increase with age, as knowledge is accumulated through the lifespan, however fluid processing ability peaks during late adolescence and then steadily declines over time (Horn et al,1981) (Figure 8.4). There is some evidence to support the value in short-term memory and cognitive training for enhancing fluid intelligence and cognitive function (Au et al, 2015).
It is expected that overall intellectual ability is maintained until at least 75 years of age and for many individuals, much longer than that. After age 70 however, “normal” declines in 1) central processing, 2) fluid intelligence, and 3) memory play a role in affecting cognitive functioning.
Despite what is known about the aging process and cognition, it is unclear why some older adults maintain their intellect and continue to be active and engaged in the world, while others disengage and/or show signs of dementia. There is evidence however, that exercise, particularly aerobic exercise can mediate the age-related changes in the brain that negatively affect cognition. (Gomez-Pinilla & Hillman, 2013).
Memory
In addition to the processes of attention and learning, cognition, knowledge and intelligence requires memory. Memory is the ability of the mind to encode, store and retrieve information. It gives us the capacity to learn and adapt from previous experiences and the power to develop skills and habits from those experiences. Memory can be classified as short-term or long-term. Short-term memory is the ability to remember and process information at the same time. Sometimes referred to as working memory, short-term memory holds only a small
amount of information in the active mind for a short period of time. Typically this is limited to seven or less items for less than a minute. This information will not be retrievable unless a conscious effort is made to retain it. This can be done through repetition or by linking the information to already available long-term memories. This suggests that at the end of a day when people can’t remember what they had for breakfast, it’s probably because they didn’t make a conscious effort to retain that information. Thus, it’s really not a short-term memory impairment (Cowan, 2008).
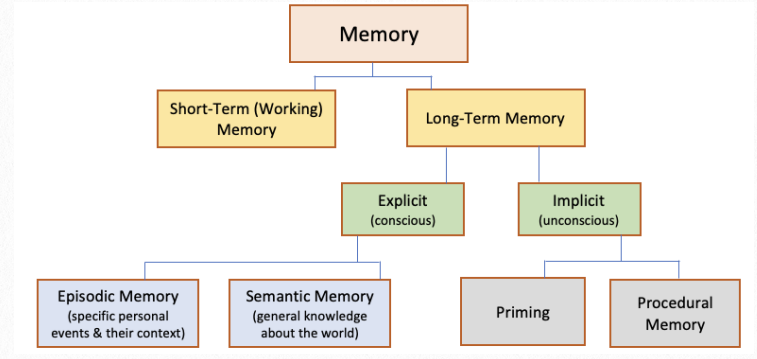
Figure 8.5 Types of Memory
Long term memory is anything remembered that took place more than a few minutes ago. The memories can last for a day or two, or for many years. There are a few ways to categorize long-term memory. Implicit memory is sometimes referred to as automatic or unconscious memory. This type of memory uses past experiences no matter how long ago they occurred, to remember things without thinking about them. A subset of implicit memory is procedural memory, which enables people to perform many everyday physical activities such as walking
and riding a bicycle. Many implicit memories are dependent on the cerebellum and basal ganglia because they are procedural in nature and involve motor skills. Implicit memories can also result from priming, which unconsciously occurs when words, or words and objects are habitually paired together. When presented with the phrase “bread and _____”, most people will respond with “butter” due to priming.
Another type of long term memory is explicit memory. Sometimes referred to as declarative memory, these thoughts require a conscious effort to recall and explain them. Tasks such as remembering what was taught in a classroom situation, who ran for president during the last election, and the date of your next dentist appointment all require the use of explicit memory.
Episodic memories are a type of explicit memory and refer to experiences or episodes that have occurred in one’s life. An example of an episodic memory is recalling the time you won a sports, scholastic, art or music competition. Semantic memory on the other hand, does not need to be experienced. This is a type of long term member that relates to facts and general knowledge.
Long-term memories are not of equal strength. The stronger they are, the more easily retrievable they are. Weaker memories often come to mind only with prompting or reminding. Long-term memories can also change over time. The memory can be merged with another and thereby be altered. Or, by repeating the memory aloud it can be influenced by the
reaction or information provided by others. Because memories are not rigid, they may not always be accurate or reliable.
As cognition and memory develops in young children ages three-five, so does their awareness of past, present and future. Between the ages of five – seven children begin to relate past and present memories more efficiently. By the time children are nine -ten years of age, they can begin to think about remembering. This “meta-memory” allows children to prepare for tests by being able to review what they know and remember versus what they don’t know.
Adult and Older Adulthood
The normal aging process includes changes in cognition, yet the heterogeneity among adults make the degree and rate of change difficult to predict. One possible contribution to the individual differences in cognitive ability observed during older adulthood is prior cognitive ability. Leibovicki and colleagues (1996) found that in adults older than 75, language
and secondary memory (delayed and prose recall) are more resistant to decline in a high-education group compared to a low-education group. Yet, attention, implicit memory and visuospatial skills were found to decline regardless of education level. Other factors relate to physical health and lifestyle (Deary et al, 2009). For example, given the delicate relationship between the circulatory system and the brain, any cardiovascular pathology may affect normal brain functioning. Indeed, risk factors present for coronary heart disease and known peripheral artery disease appear to be associated with poorer memory and executive functions. When health status is controlled, some cognitive abilities, such as vocabulary remain intact during the aging process and can even improve. However, other abilities such as reasoning, memory and processing speed decline over time (Harada et al, 2013).
One of the most common cognitive complaints among middle-aged and older adults is that they can’t remember as well as they use to. In fact, older adults don’t perform as well as younger adults on memory tasks. Researchers have found that memory impairments may be related to slowed processing speed, reduced ability to ignore irrelevant information, and decreased use of strategies to improve learning and memory (Harada et al, 2013).
Not all types of memory are affected the same during normal aging. For example, episodic memory declines across the lifespan, while semantic memory declines much later in life and implicit memory remains completely intact. The process of acquisition, which is the ability to encode new information into memory becomes slower across the lifespan
whereas retention of information that is successfully learned is preserved in healthy older adults. Nevertheless, a decline in the ability to retrieve new information is observed in older adults (Harada et al, 2013).
In addition to changes in memory, older adults are known to experience alterations in attention. Simple auditory attention span shows only a slight decline in later life, however age plays a negative role in divided and selective attention. Divided attention is the ability to focus on multiple tasks simultaneously. Selective attention is important for driving a car in which the driver needs to focus on relevant information in the environment while ignoring other information (Harada et al, 2013).

8.5 Older Men Playing Chess
Executive functioning includes a range of cognitive skills such as the ability to plan, organize, judge, reason and problem-solve. There is evidence that older adults, especially those older than 70, tend to think more concretely than younger adults, due to challenges in abstraction and mental flexibility (Oosterman, 2010; Salthouse 2010). In addition, reasoning with unfamiliar material declines with age and yet, other skills such as reasoning with familiar material and the ability to appreciate similarity and describe the meaning of proverbs, remain consistent across the lifespan (Harada et al, 2013). Research findings suggest that cognitive training can help older adults perform better on cognitive testing for many years (Willis et al, 2006).
It should be kept in mind that normal age-related cognitive changes do not impair an individual’s ability to function. If an otherwise healthy older adult does develop functional impairments, even with complex tasks such as managing finances, the best course of action is to seek a medical examination. Sensory impairments such as vision or hearing problems, dehydration, dietary issues such as a B12 deficiency, adverse reactions to medication, and a new illness can all affect cognitive functioning. If a medical cause for impaired cognition cannot be identified then a work-up for dementia is warranted.
Final Thoughts
Normal aging is associated with declines in certain cognitive abilities. Nevertheless, the declines are small and should not interfere with any activities of every day functioning and most types of work. Despite being a severe burden on families and society, dementia is not an inevitable condition of older adulthood. Regular physical exercise, intellectual endeavors and social engagement are all activities associated with high cognitive function in older adults.
References
Au, J., et al. (2015). Improving fluid intelligence with training on working memory: a meta-analysis. Psychonomic Bulletin and Review, 22(2), 366-377.
Cattell, R. B. (1963). Theory of fluid and crystallized intelligence: A critical experiment. Journal of Educational Psychology, 54(1), 1-22.
Chi, M. T., & Ohlsson, S. (2005). Complex declarative learning. Cambridge handbook of thinking and reasoning. Cambridge University Press.
Cowan N. (2008). What are the differences between long term, short-term, and working memory? Progress in Brain Research, 169, 323–338. https://doi.org/10.1016/S0079-6123(07)00020-9
Gomez-Pinilla, F., & Hillman, C. (2013). The influence of exercise on cognitive abilities. Comprehensive Physiology, 3(1), 403-428.
Harada, C.N., Natelson Love, M.C., Triebel, K. Normal cognitive aging. Clinics in Geriatric Medicine, 29(4), 737-752.
Horn, J. L., Donaldson, G., & Engstrom, R. (1981). Apprehension, memory, and fluid intelligence decline in adulthood. Research on Aging, 3(1), 33-84.
Leibovicki, D., Ritchie, K., Ledesert, B., Touchon, J. (1996). Does education level determine the course of cognitive decline? Age and Ageing, 25, 392-397.
Oates, J., & Grayson, A. (Eds.). (2004). Cognitive and language development in children. Blackwell Publishing; Open University Press, 2004
Oosterman, J. M. et al. (2010). Assessing mental flexibility: neuroanatomical and neuropsychological correlates of the Trail Making Test in elderly people. The Clinical Neuropsychologist, 24, 203-219.
Rafnsson, S.B., Deary, I.J., Fowkes, F.G.T. (2009). Peripheral arterial disease and cognitive function. Vascular Medicine, 14, 51-16.
Rafnsson, S.B., Deary, I.J., Smith, FB, Whiteman, M.C., Fowkes, F.G.T. (2007). Cardiovascular diseases and decline in cognitive function in an elderly community population: the Edinburgh Artery Study. Psychosomatic Medicine, 69, 425-434.
Salthouse, T.A. Decomposing age correlations on neuropsychological and cognitive variables. Journal of the International Neuropsychological Society, 5, 650-661.
Schneider, W. J., & McGrew, K. S. (2012). The Cattell-HornCarroll model of intelligence. In D. Flanagan & P. Harrison (Eds.), Contemporary intellectual assessment: Theories, tests, and issues (3rd ed., pp. 99–144). New York: Guilford.
Steinberg, L. (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69-74.
Willis, S.L., Tennstedt, S.L., Marsiske, M., et al. (2006). Longterm effects of cognitive training on everyday functional outcomes in older adults. Journal of the American Medical Association, 296, 2805-2814.
For more details about the Cattell-Horn-Carroll (CHC) Model of Intelligence v2.2, go to http://www.iapsych.com/chcv2.pdf
Images
Title page. Brain. Courtesy of Pacific Northwest National Laborary. Retrieved from: https://wordpress.org/openverse/image/d8790ab1-c538-491a-9666-fac997712a65
Figure 8.3 Child Applying Cognitive Concepts While Building. Photo by Yagazie Emezi Retrieved from: https://www.imagesofempowerment.org/pa-1799312_450
Figure 8.4 Fluid and Crystallized Intelligence Across the Lifespan. Tracy Ramsay, author. Retrieved from https://commons.wikimedia.org/wiki/File:Fluid_intelligence_decline.jpg
Figure 8.5 Older Men Playing Chess. Retrieved from https://www.nia.nih.gov/health/how-aging-brain-affects-thinking
