1 The Biomedical Data Journey: Research Process, Infrastructure, and Ethics
Reading Objectives
After reading this chapter, you should be able to:
- Explain how a broad research topic becomes a research question, hypothesis, and study design, including the roles of explanatory, outcome, demographic, and contextual variables.
- Distinguish observational from experimental studies and explain why observational associations, including those observed over time, do not by themselves establish causation.
- Describe the biomedical data journey from study design and participant encounters through data capture, processing, documentation, controlled access, analysis, and responsible reuse.
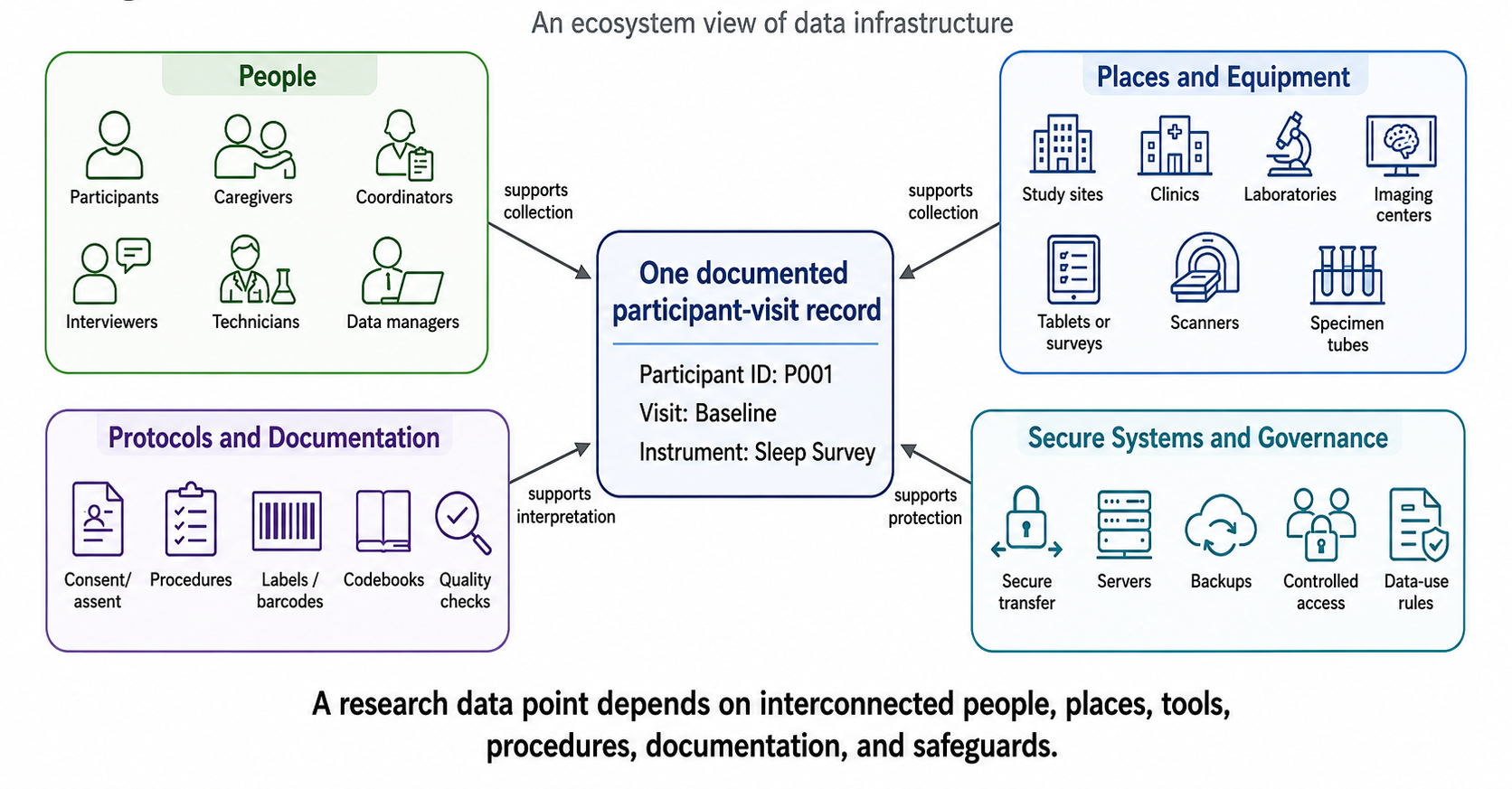
- Explain how data infrastructure shapes research data, including the roles of participants, caregivers, staff, study sites, instruments, laboratories, identifiers, secure transfer, storage, and quality-control procedures.
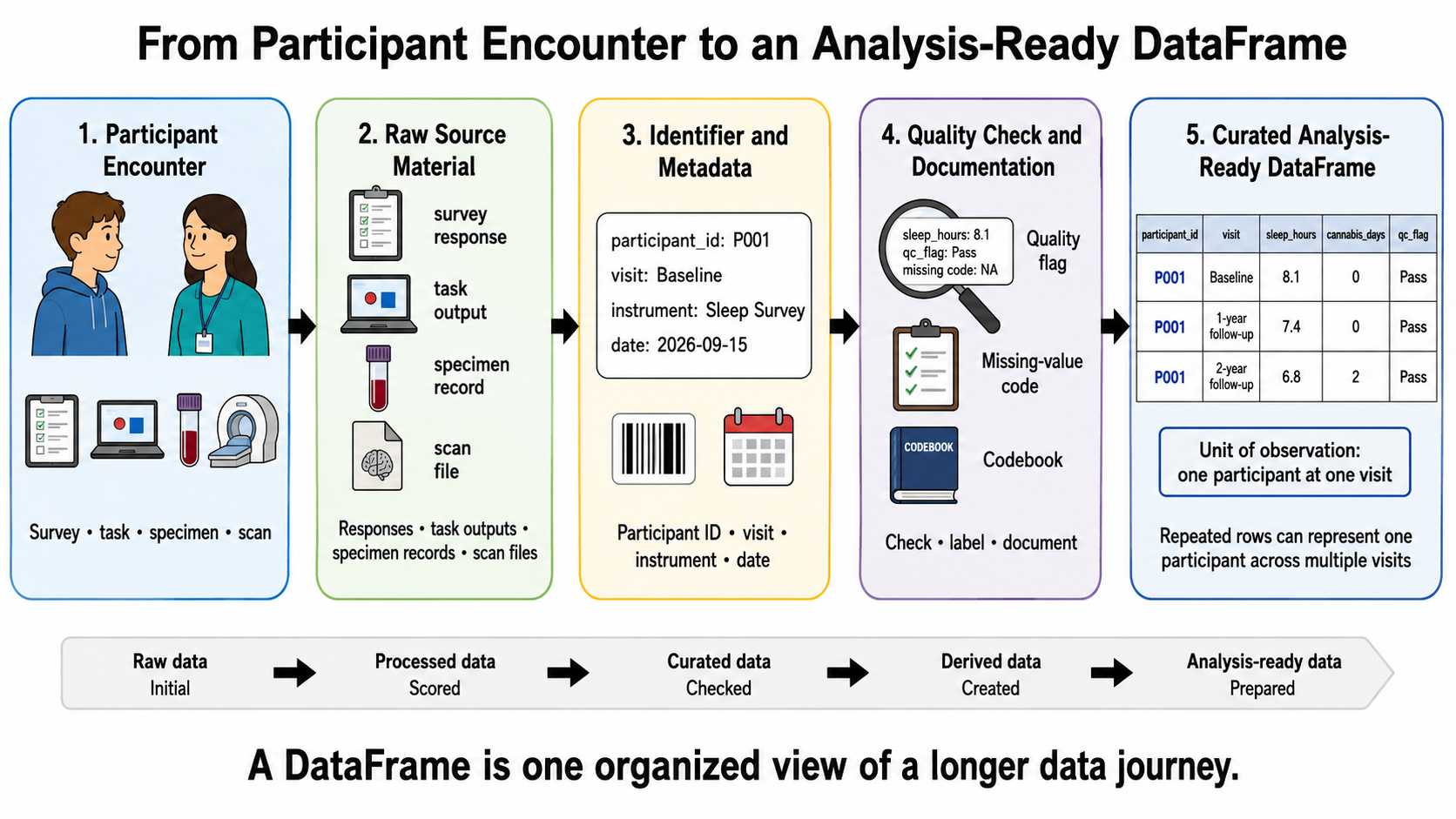
- Interpret the basic structure and documentation of a biomedical dataset, including DataFrames, units of observation, participant and visit identifiers, metadata, data dictionaries, codebooks, provenance, and data states.
- Apply foundational principles of ethical and responsible data use, including privacy, confidentiality, re-identification risk, controlled access, data-use agreements, secure storage and deletion, responsible interpretation of race and ethnicity variables, and appropriate citation and acknowledgment.
- Explain why reproducible notebook workflows and synthetic data support responsible learning and analysis, while distinguishing reproducibility from correctness, causal validity, or replication.
Key Terms
Biomedical data journey; data governance; data infrastructure; hypothesis; research question; study design; variable.
Introduction: From Research Questions to Analytic Datasets
Substance use and related harms are often reduced to matters of personal choice or morality. Such narratives overlook the many influences that shape behavior and health, including development, family and peer environments, stress, opportunity, policy, biology, and access to resources. When people who use substances are blamed for “bad choices,” important social and structural factors remain invisible and stigma grows. This course begins from a broader, evidence‑based view – questions about addiction and health require attention to multiple influences and careful data collection.

Scientific inquiry starts with questions rather than assumptions. Researchers ask how elements of a young person’s environment relate to later outcomes—for example, how neighbourhood social support or sleep quality relates to substance use, or how stress and peer relationships shape development. Such questions cannot be answered by inspecting a spreadsheet alone. They call for a process that spans study design, measurement, data collection, curation, analysis, and ethical governance. Data do not appear spontaneously; they are created through an organised journey.
A value in a dataset might originate in a youth’s survey response, a caregiver interview, a computer‑based task, a laboratory analysis of a specimen, or a brain‑imaging session. That value may be collected by a research coordinator, interviewer, technician, or clinician. It may be checked for quality, assigned an identifier, linked to documentation, transferred through secure systems, and stored under rules that limit who can access it and how it may be used. Every row in a dataset has a history.
Before researchers can analyze data, they must make a series of deliberate decisions – decide what they want to understand; design a study that can address the question; determine which people and experiences to include; select ways to measure important concepts; protect participants and their information; and document how the resulting data should be interpreted. These choices shape every later step and must be revisited when interpreting results.
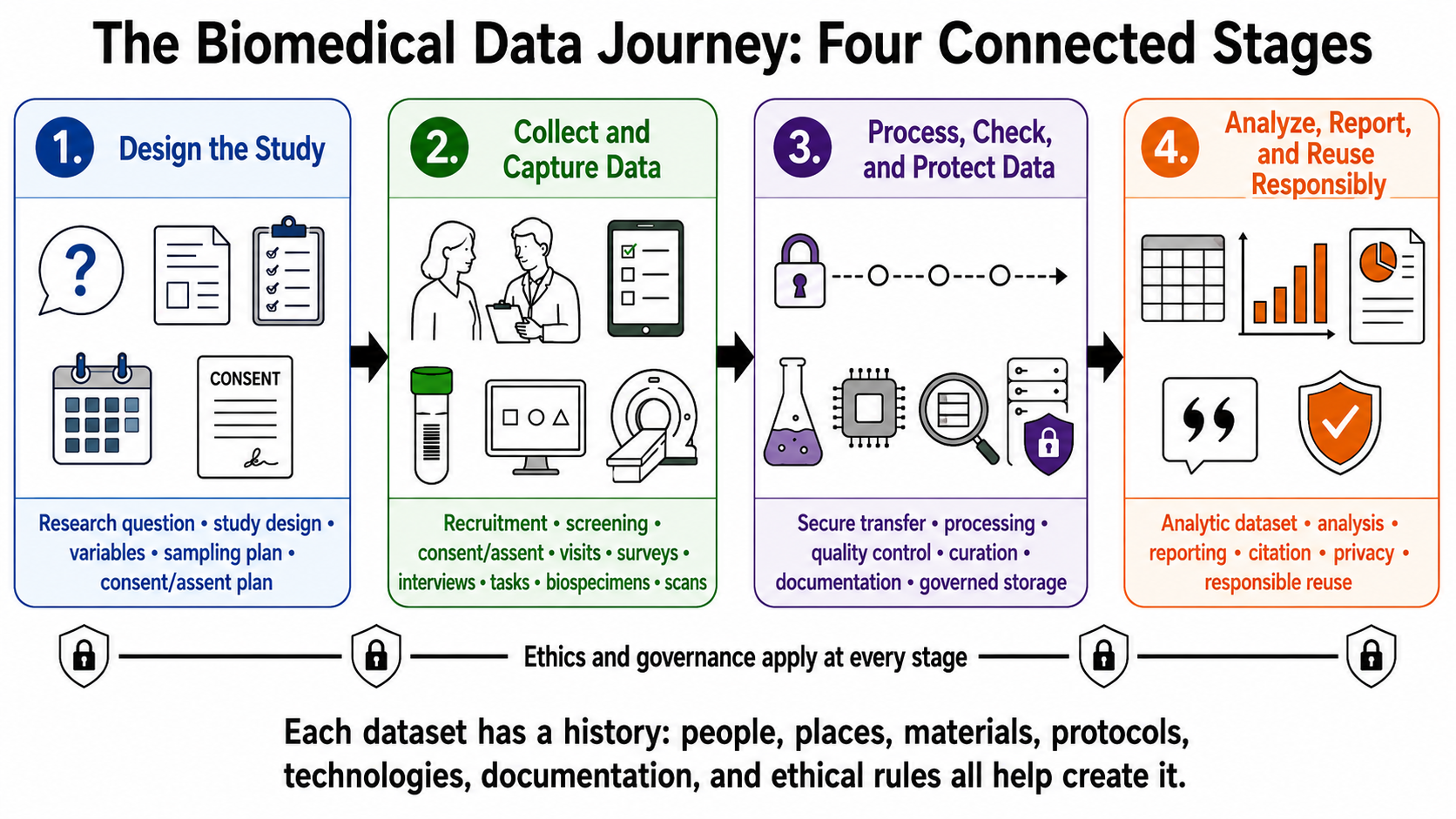
The biomedical data journey provides a framework for tracing this process. It highlights four connected stages: (1) framing and designing the study; (2) recruiting participants and collecting data; (3) processing, checking, and documenting the data; and (4) governing, analyzing, reporting, and responsibly reusing data. Each stage builds on those that precede it. A change in recruitment, measurement, or documentation influences what analysts can do later. Figure 1.2 illustrates these stages, reminding us that the rows and columns seen in a DataFrame are the end product of a long chain of human, technical, and ethical decisions.
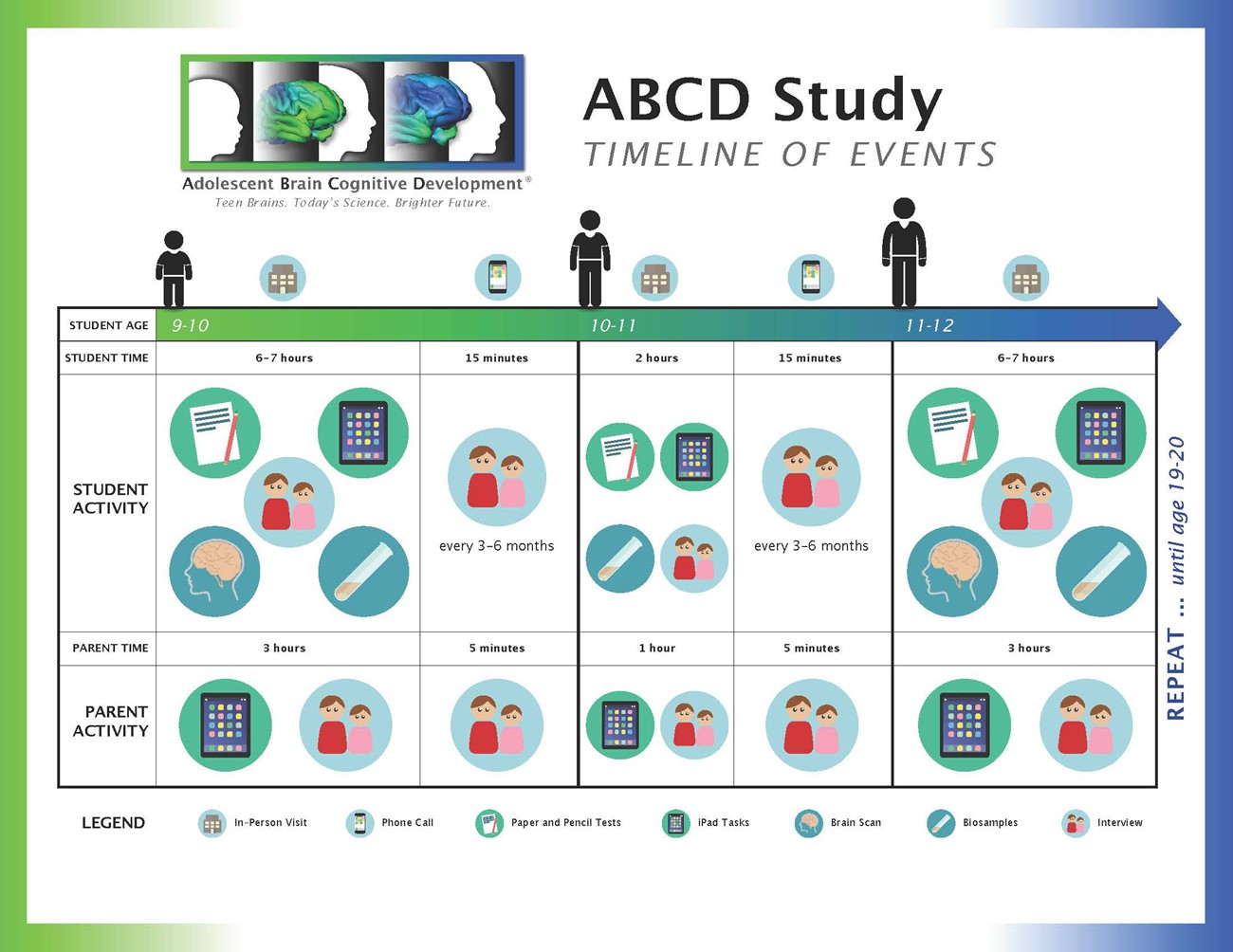
Throughout this course we will return to the Adolescent Brain Cognitive Development (ABCD) Study as a running example. ABCD is a large, multisite longitudinal study that follows more than 11,000 children across 21 sites for a decade, collecting data on health, behaviour, cognition, social environment, substance use, biological measures, and brain development. Its scale and multimodal design enable questions that no single survey, clinic, or laboratory could answer. At the same time, its complexity means that analysts must know what each variable represents, who provided it, when and how it was collected, what the possible values mean, whether data are missing, and what the study design can and cannot support. Sensitive information about young people, families, health, substance use, genetics, and brain development carries ethical responsibilities.
This chapter establishes foundational concepts for DSARM 1. You will learn how broad topics become research questions, how theory leads to constructs, measures, and variables, and how hypotheses are formulated and tested. You will learn the difference between exploratory and confirmatory questions, and between explanatory, outcome, demographic, and contextual variables. You will examine study designs (observational versus experimental, cross‑sectional versus longitudinal), sampling and recruitment, and the basic structure of a DataFrame. You will see why observational studies can identify important patterns but do not alone establish causation. You will explore the physical and digital infrastructure that makes data possible, the documentation that enables interpretation, and the ethical principles that govern responsible data use.
2. From Question to Study Design
2.1 From Broad Topics to Specific Questions
Health researchers often begin with a broad topic, such as youth development and substance use. A topic captures a general area of curiosity, but it does not yet specify what will be measured or how relationships will be tested.
To make progress, researchers refine that topic into a research question: an inquiry that identifies relationships, patterns, descriptions, or changes that can be investigated empirically.
A scientific research question always includes variables. For example, instead of asking:
How do teenagers grow up?
An addiction research project might ask:
How is neighborhood social support related to later cannabis use among adolescents?
This question identifies a population, proposes a relationship between two variables, and invites data collection.
Broad topics and research questions emerge from theory and prior evidence. Theory explains why certain relationships might exist. Constructs are the abstract concepts that theory proposes. Measures translate constructs into observable quantities. Variables are the measured values we analyze.
Each step should be explicit:
Theory → Construct → Measure → Variable
For instance, the construct stress might be measured by a validated questionnaire or a biomarker. A research question might then connect stress as an explanatory variable to another variable, such as sleep quality, as the outcome variable.
When a relationship is expected, researchers often formulate a hypothesis: a specific, testable prediction that can be falsified.
2.1.1 Exploratory and Confirmatory Questions
Research questions come in two main forms.
Exploratory questions ask broadly about patterns or associations without specifying which variables explain which outcomes. For example:
What factors most influence substance use among urban high school students?
Exploratory work is common when relationships have not been extensively studied. It allows researchers to examine large datasets, identify patterns, and generate new hypotheses.
Confirmatory questions test specific relationships derived from theory or prior evidence. For example:
Does peer support reduce risk of substance use among urban high school students?
This confirmatory question proposes a direction of effect between a predictor and an outcome. It may lead to a hypothesis such as:
Adolescents with higher peer support will show lower substance use frequency over the next year compared with those with lower peer support.
Exploratory questions are useful for discovery. Confirmatory questions enable rigorous testing of hypotheses.
2.1.2 Explanatory, Outcome, Demographic, and Contextual Variables
Researchers classify variables by their role in a question.
An outcome variable is the focus of a question. It represents the result to be explained. It is sometimes called a dependent variable or response variable.
An explanatory variable is expected to influence the outcome. It is often called an independent variable or predictor.
Demographic variables describe characteristics of participants, such as age, gender, race, or socioeconomic status.
Contextual variables capture features of the environment, such as family, neighborhood, school, policy, or historical context, that may shape outcomes.
For example, if a study asks how weekly cannabis use is related to academic performance, then weekly cannabis use is the explanatory variable and academic performance is the outcome variable. Participants’ age and neighborhood deprivation could be demographic and contextual variables, respectively.
The ABCD Study, which follows more than 11,000 young people across 21 sites for ten years, provides many examples. A broad topic might be:
Adolescent brain development and substance use.
A research question could ask:
How does sleep quality in early adolescence relate to later cognitive performance?
In this question, sleep quality is the explanatory variable. It might be measured by actigraphy or self-report. Cognitive performance is the outcome variable. It might be measured by standardized tests.
Demographic and contextual variables could include age, sex, family income, and parental education. Because ABCD collects repeated measures over a decade, researchers can investigate change over time.