
7 Public Policy & Addiction
Reading Objectives
- Criminalization and Mass Incarceration: Analyze how punitive policies—including the War on Drugs and deterrence theories—have contributed to mass incarceration and racial disparities in drug-related arrests and imprisonment.
- Prevention, Recovery, and Public Health: Evaluate the evolution from abstinence-only models to comprehensive public health strategies (including harm reduction and treatment-based approaches) and their impact on addiction outcomes.
- Markets, Legalization, and Regulation: Examine the regulation and structure of markets for potentially addictive substances, focusing on supply- and demand-side policies, corporate influence, and market control measures.
Key Terms
- Public Policy: Government actions through laws, regulations, funding, and enforcement to address societal challenges and manage public resources.
- Criminalization: The process of converting behaviors—such as drug use—into criminal offenses subject to legal sanctions.
- Deterrence Theory: The idea that individuals will refrain from criminal behavior if the anticipated costs (e.g., punishment) exceed the benefits.
- Harm Reduction: A public health approach that minimizes the negative consequences of drug use without requiring complete abstinence.
- Supply-Side Policies: Strategies that reduce the availability of addictive substances by regulating their production, distribution, or sale.
- Demand-Side Policies: Measures aimed at decreasing the desire or ability to use addictive substances, often through taxation, education, or treatment.
- Regulation: The enforcement of rules and standards by government agencies to control behaviors and ensure public safety.
- Market Structure: The organization and competitive dynamics within a market, including the number and size of firms and the distribution of market power.
Introduction to Public Policy and Addiction
In the late 1990s, Purdue Pharma, a pharmaceutical company owned by the Sackler family, launched an aggressive marketing campaign promoting OxyContin as a safe and effective solution for chronic pain, claiming less than a 1% risk of addiction. However, these claims
were misleading and based on inadequate evidence. Purdue’s relentless push dramatically increased opioid prescriptions—from $44 million in sales in 1996 to nearly $3 billion by 2002—exposing millions of Americans to highly addictive substances. This aggressive corporate practice ignited what became the devastating U.S. opioid epidemic, characterized by widespread addiction, overdose deaths, and social upheaval.
Public policy initially lagged behind these market forces, allowing Purdue and other pharmaceutical companies to market opioids with minimal oversight. Eventually, as the scale of the crisis became apparent, policymakers responded with legal actions against Purdue and similar firms, imposing billion-dollar settlements and reforms to industry practices. The Purdue Pharma case vividly illustrates how regulatory frameworks, market incentives, corporate interests, and public health concerns intersect, highlighting the profound impact that public policy decisions—or the lack thereof—can have on addiction epidemics.
Public policy refers to the actions governments take—through laws, regulations, funding decisions, and enforcement—to address societal problems, achieve collective goals, and manage public resources. Policies determine not only which substances are legally available, but also how they are marketed, distributed, taxed, and regulated, directly shaping both the social environment and the public’s health. Addiction represents a critical public policy issue because its consequences extend beyond individual health, affecting communities through increased healthcare costs, lost productivity, family disruption, and crime. The addictive potential of substances, combined with social determinants such as poverty, inequality, and trauma, makes addiction a complex issue requiring multifaceted policy responses.
This chapter explores several key policy debates related to addiction. It examines the history and impact of criminalization approaches exemplified by the “War on Drugs,” evaluating their consequences for incarceration rates and racial inequality. It discusses alternative public health strategies, such as harm reduction and treatment-based policies, aimed at mitigating addiction-related harms rather than punishing substance users. Additionally, it analyzes ongoing debates surrounding the regulation and structure of markets for addictive substances—considering how supply-side controls (e.g., prescription limits and interdiction efforts) and demand-side measures (e.g., taxation and education) interact. Through case studies and current data, including variables from the ABCD dataset, this chapter assesses how effective policy can reduce addiction-related harms, hold corporations accountable, and promote healthier communities.
Criminalization: The War on Drugs and Mass Incarceration

Should drug use and addiction be addressed primarily through criminal punishment or treated as public health issues requiring supportive interventions? The criminalization approach treats drug use and addiction primarily as criminal offenses. It reached its peak intensity during the U.S. “War on Drugs” launched in the 1980s. This punitive strategy (punitive means intending to punish) led to an intensification of arrests and imprisonment and particularly for drug offenses. In 1980, approximately 503,586 individuals were incarcerated, equating to an incarceration rate of 220 per 100,000 residents. By 2008, this number peaked at over 2.3 million, with a rate of 755 per 100,000 residents (Kang-Brown et. al. 2020).
Drug offenses accounted for a large share of the rise in imprisonment. By calculations of legal expert Michelle Alexander, by 2010, drug offenders in federal prison had increased to 500,000 per year, up from 41,000 in 1985; drug related charges accounted for more than half the rise in state prisoners between 1985 and 2000. In contrast, according to criminologist John Pfaff, the percent of state prisoners whose primary offense was drug-related peaked at 22% in 1990. Whichever interpretation of the statistics, the United States has led the world in both incarceration and drug-related arrests and incarceration (Institute for Crime & Justice Policy Research 2025).
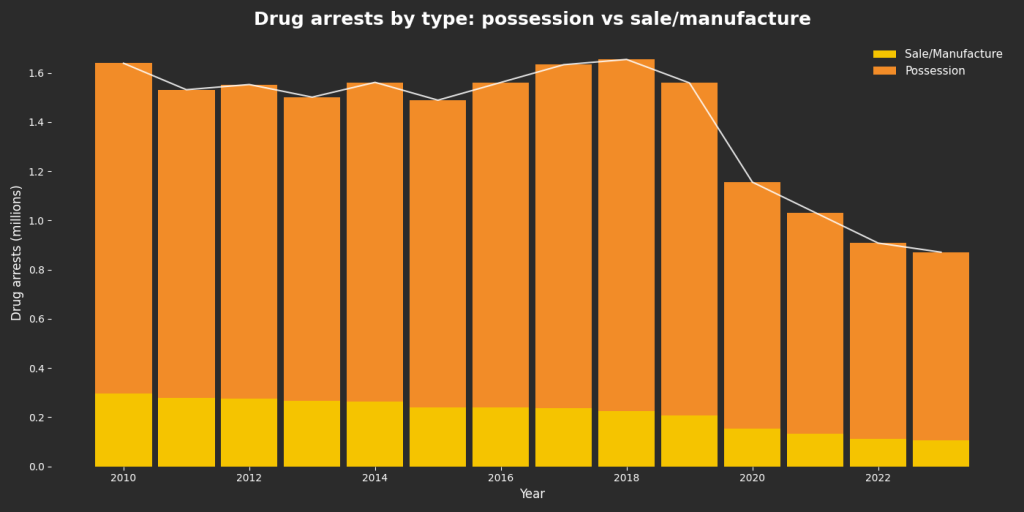
Stacked bars display annual drug arrests disaggregated by offense type using FBI Uniform Crime Reports data. In every year shown, arrests for possession substantially exceed arrests for sale or manufacture. Total drug arrests remained relatively stable through the 2010s before declining sharply beginning in 2020. Data Source: Federal Bureau of Investigation (FBI), Uniform Crime Reports (UCR), Crime in the United States, annual arrest tables (Drug Abuse Violations).
Deterrence & Rational Choice Theory
The criminalization paradigm is grounded in a belief that deterrence and punishment will reduce drug use. It views illicit drug use as a crime to be suppressed through enforcement. This approach was fueled in part by moral models of addiction (seeing drug use as a personal failing) and by public fears about drugs in the 1980s (e.g. the crack cocaine epidemic). Policies like mandatory minimum sentencing and “three strikes” laws reflected a theory that swift, certain, and severe punishment would deter individuals from using or selling drugs. Here, “deterrence” is a latent construct—inferred from patterns of arrests and incarceration rather than directly measured, and operationalized through indicators like sentence length or arrest rates. Deterrence theory assumes Rational Choice Theory.
Rational Choice Theory posits that individuals make decisions by weighing the potential benefits and consequences of their actions. Originating from classical utilitarian
philosophy, notably the works of Cesare Beccaria and later expanded by economists like Gary Becker (1968), this theory suggests that criminal behavior results from a calculated decision-making process where the perceived rewards outweigh the risks. In the context of drug-related offenses, Rational Choice Theory implies that individuals engage in drug use or trafficking after assessing the potential gains against the likelihood and severity of punishment. Policies based on this theory aim to deter such behaviors by increasing the perceived risks through stringent laws and penalties.
Criticisms of Deterrence Theory
Research has found that increasing the severity of punishment has little deterrent effect on substance use behavior. Studies have consistently found (including analyses by the National Institutes of Health and Pew Research Center) no statistically significant relationship between higher drug imprisonment rates and lower levels of drug use, drug overdose deaths, or drug arrests (Nagin 2013; Pew Research Center 2011). In other words, locking up large numbers of drug offenders has not produced the intended public health benefits in terms of reduced addiction or harm.
Mass Incarceration and the Politics of Race and Racism
In her influential book, The New Jim Crow, Michelle Alexander (2010) argues that the War on Drugs served as a tool of racialized social control, disproportionately targeting Black and Latino communities despite similar rates of drug use across racial groups. Alexander contends that drug criminalization became a key mechanism for maintaining racial inequalities after the civil rights era, effectively creating a new racial caste system through mass incarceration and the resulting collateral consequences.
Marijuana arrests also illustrate how policy reforms can change enforcement patterns while racial disparities persist. As shown in Figure 3, adult cannabis possession arrest rates were consistently higher for Black adults than for White adults across legalization, decriminalization, and no-policy-change states. In states that implemented legalization, the arrest rate in 2008 was 599.2 for Black adults and 210.9 for White adults, and by 2019 it fell to 38.0 and 15.9, respectively (Sheehan et al., 2021). In states that decriminalized, arrest rates declined as well, from 810.0 (Black adults) and 220.0 (White adults) in 2008 to 361.4 and 102.9 in 2019, while in states without a policy change, arrest rates remained very high for Black adults (818.5 in 2008; 771.0 in 2019) and were lower and more stable for White adults (203.3 in 2008; 170.3 in 2019).

Alexander emphasizes that these disparities are not coincidental but systemic, rooted in biased enforcement and sentencing policies. The intense policing of minor drug offenses, notably marijuana, resulted in millions of disproportionately Black and Latino individuals entering the criminal justice system. This racialized enforcement has profound social and health implications, perpetuating cycles of poverty, family disruption, and adverse community conditions, exacerbating social determinants of health linked to addiction and poor outcomes.
Ultimately, Alexander’s analysis reveals that the War on Drugs was less about curbing drug use and more about controlling marginalized racial groups, illustrating how ostensibly race-neutral policies can operate with deeply racialized consequences.
Summary: Criminalization: The War on Drugs and Mass Incarceration
The criminalization of drug use, exemplified by the War on Drugs, significantly increased incarceration rates but failed to effectively reduce substance use or addiction. Instead, punitive policies disproportionately targeted Black and Latino communities, exacerbating racial inequalities and creating enduring social harms without achieving the intended public health outcomes.
Prevention, Recovery, and Public Health
Central to public policy debates on addiction is the question: What should public policy and public money be spent on for addiction prevention, recovery, and public health initiatives? The discussion centers around whether resources should primarily focus on punitive enforcement, abstinence-based prevention programs, or more comprehensive public health strategies including harm reduction, treatment, and social support.
From “Just Say No” to Harm Reduction
In the 1980s, U.S. drug policy was dominated by the “Just Say No” ethos, spearheaded by First Lady Nancy Reagan. This campaign relied on moral messaging, scare tactics, and punitive measures. Programs like D.A.R.E. (Drug Abuse Resistance Education) and zero-tolerance school policies aimed to prevent drug use by instilling an absolutist message against any drug involvement. However, extensive research later revealed that these abstinence-only approaches had little lasting effect on youth drug use behavior, as they neglected the complex social, psychological, and economic factors underlying addiction (Ennett et al., 1994).
In contrast to punitive strategies, the harm reduction approach aims to mitigate the negative consequences of drug use without necessarily requiring abstinence. Harm reduction emerged in the late 20th century as a pragmatic public health response—initially gaining traction in Europe during the HIV/AIDS epidemic and later gradually in North America. This approach is grounded in behavioral science insights that many people with addiction are unable or unwilling to immediately quit, and that meeting people “where they are” can save lives and improve health (Marlatt, 1996). Rather than moralizing or criminalizing drug use, harm reduction focuses on reducing infectious disease transmission, preventing overdose deaths, and linking users to social and medical services.
Examples of Harm Reduction Interventions include:
- Needle and Syringe Exchange Programs (SEPs): Providing sterile syringes dramatically reduces HIV and hepatitis C transmission.
- Opioid Substitution Therapy (OST): Medications like methadone or buprenorphine stabilize opioid-dependent patients, reducing illicit drug use and overdose risk.
- Naloxone Distribution: Equipping law enforcement, community members, and peers with naloxone effectively reverses opioid overdoses.
- Supervised Consumption Sites: Facilities where drug use occurs under medical supervision, minimizing fatalities and facilitating treatment access.
- Drug Checking Services: Testing street drugs for dangerous contaminants like fentanyl prevents accidental overdoses.
These measures not only immediately reduce harm, but also serve as critical entry points into broader healthcare and recovery pathways.
Social Determinants of Health and Harm Reduction
Harm reduction policies explicitly address social determinants of health (SDH). They recognize that environmental factors—such as poverty, homelessness, and systemic marginalization—increase health risks among drug-using populations. For instance, unstable housing correlates with riskier injection practices and higher overdose rates; harm reduction measures like safe injection sites and housing-first interventions can mitigate some immediate dangers associated with social disadvantage, though they do not fully resolve underlying issues.
In parallel to harm reduction, a broader public health perspective has reshaped addiction policy, treating substance use disorders as chronic health conditions rather than moral failings or criminal behaviors. This paradigm emphasizes prevention by addressing underlying risk factors, integrating addiction treatment into mainstream healthcare, and diverting individuals away from the criminal justice system into treatment-based solutions (e.g., drug courts, deflection programs). Further, insights from social and behavioral sciences underscore addiction as symptomatic of deeper underlying factors, including trauma, mental illness, social isolation, and economic stress. This has led to holistic treatment approaches incorporating trauma-informed care, given that adverse childhood experiences (ACEs) significantly elevate addiction risk.
Policy Landmarks Supporting Public Health Approaches
Recent legislative measures cement the public health shift. The Mental Health Parity and Addiction Equity Act of 2008 and the Affordable Care Act (ACA) of 2010 mandated insurance coverage for addiction treatment services, dramatically expanding access. Subsequent federal funding through the 21st Century Cures Act (2016) and the SUPPORT Act (2018) significantly expanded treatment and prevention capacity, reflecting a policy consensus increasingly oriented toward health rather than punishment.
Summary: Prevention, Recovery, and Public Health
Public policy has gradually shifted from punitive, abstinence-only strategies toward comprehensive public health approaches, including harm reduction and medication-assisted treatments. These strategies acknowledge addiction as a complex chronic health
condition influenced by social determinants, effectively reducing harms and providing pathways to recovery by addressing underlying causes rather than criminalizing behaviors.

Health Insurance & Behavioral Health Policy
Primer: health insurance and why it matters for addiction & mental health
Health insurance is a risk-pooling contract: people (and/or employers or governments) pay predictable premiums so that rare but expensive care is affordable when needed. Plans define covered benefits and share costs with enrollees through deductibles (what you pay before the plan pays), copays (flat fees per visit/drug), and coinsurance (a percentage of the bill). Access usually runs through provider networks—clinicians and facilities that have contracted rates. Plans also use utilization management tools—such as prior authorization, step therapy, and medical-necessity reviews—to control spending and standardize care. These non-price rules can help coordinate treatment, but when misapplied they delay or deny evidence-based care.
Public vs. private (who pays / who’s eligible)
In the United States, coverage is a mixed system.
- Private health insurance is provided by a private company (e.g., United Healthcare, Blue Cross, etc.), typically through employer-sponsored insurance and individual plans created under the Affordable Care Act (ACA).
- Public health insurance is provided by government programs, including Medicaid/CHIP (joint state–federal coverage for low-income individuals and families), Medicare (age 65+ and certain disabilities), and programs for veterans and military families (VA and TRICARE). Although there are increasing public-private arrangements of publicly funded health care (e.g., Medicare Advantage).
Why it matters for substance use and mental health (“behavioral health”)
Addiction and many mental health conditions are chronic, relapsing disorders. Outcomes depend on continuous access—screening, timely treatment initiation, and retention over months, not days. Whether a person actually reaches effective care hinges on coverage design:
- What’s covered: medications for opioid use disorder and alcohol use disorder (MAT: buprenorphine, methadone, naltrexone), psychotherapy, peer/recovery supports, crisis response (including 988-linked services), and residential or intensive outpatient care.
- Accessibility: reaching care is determined by the breadth of in-network clinicians (including child/adolescent and bilingual providers), prior authorization and other
non-quantitative limits, and out-of-pocket costs that deter starting or sticking with care.
Historically, behavioral health was undercovered and stigmatized, producing thin networks and higher patient costs than for medical/surgical care. Modern access rests on parity rules (requiring behavioral health coverage to be no more restrictive than medical/surgical) and the ACA/Medicaid scaffolding that broadened eligibility and established behavioral health as an essential benefit. In practice, the fine print of insurance—benefit definitions, network depth, and utilization rules—often decides whether clinically effective addiction and mental-health care is available in theory or accessible in reality.
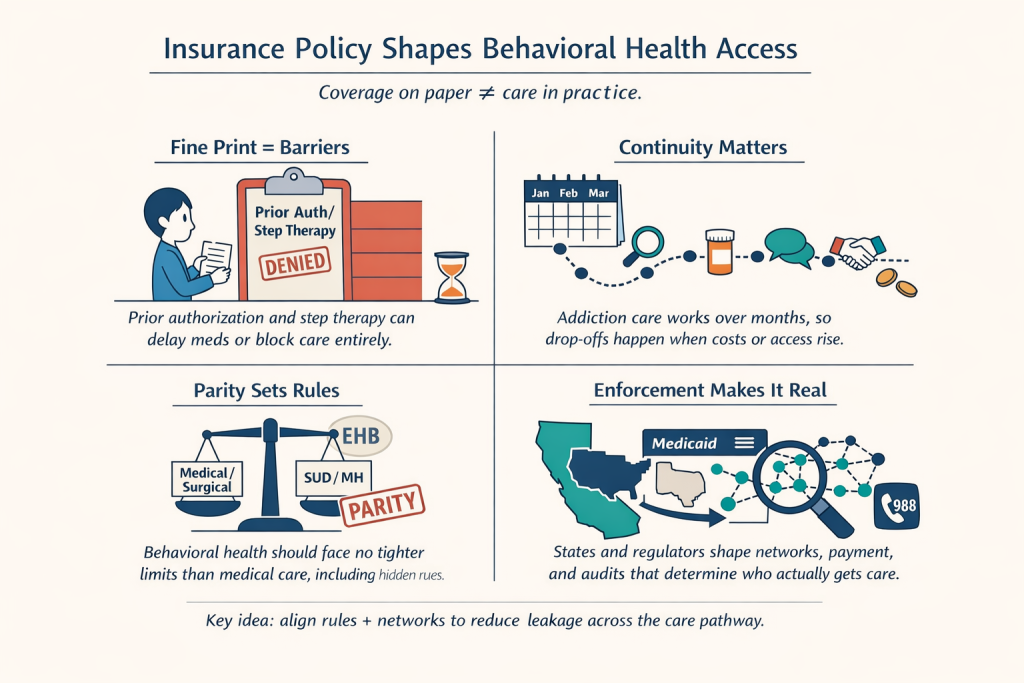
Key Policy Pillars Governing Behavioral-Health Coverage
Complex legal and administrative systems shape whether addiction and mental-health care is merely promised on paper or delivered in practice. Each policy pillar below changes the amount of your access to care — what’s covered, how easy it is to reach, and who is actually able to use it.
Federal parity & the benefits floor
The Mental Health Parity and Addiction Equity Act requires that behavioral health benefits be no more restrictive than medical/surgical benefits. Parity applies to both quantitative limits (e.g., copays, visit limits, deductibles) and non-quantitative treatment limits (NQTLs) — the fine print that shapes access: prior authorization, step-therapy requirements, medical-necessity criteria, network admission standards, provider credentialing, and fail-first rules. In short, if a plan is generous and low-friction for medical conditions, it must be equivalently generous and low-friction for SUD/MH.
The Affordable Care Act makes mental health and substance use disorder care an Essential Health Benefit in the individual and small-group markets, extends parity into those markets, bans pre-existing condition exclusions, and broadens eligibility and purchasing via Medicaid expansion and the Marketplaces. Together, MHPAEA + ACA create the national baseline: behavioral health must be covered, and it must be covered on terms comparable to medical/surgical care.
Medicaid/Medicare specifics
For low-income adults, Medicaid is the dominant coverage source for SUD/MH. Expansion states cover more people and typically include a broader behavioral-health benefit. But benefit design, delivery (often managed care), and payment rates are state-dependent, which is why access looks different across state lines.
Federal Medicaid generally will not pay for adult inpatient SUD/MH care in large facilities (the Institution for Mental Diseases rule). States can use Section 1115 waivers to finance residential treatment within specified guardrails (length of stay, quality reporting, transitions to outpatient), partially softening a long-standing barrier for higher-acuity care.
The Early and Periodic Screening, Diagnostic, and Treatment requirement guarantees comprehensive screening and all medically necessary treatment for children and adolescents. For behavioral health, EPSDT is a powerful entitlement: it compels coverage of needed services even if they aren’t explicitly listed in a state’s plan.
Medicare covers outpatient psychotherapy, psychiatric services, partial hospitalization/intensive outpatient, and SUD treatments, with program-specific billing rules. Payment policy (rates, tele-behavioral flexibilities, collaborative care codes) strongly influences network depth—which specialties participate and how quickly older adults can get care.
Enforcement & market conduct
Parity isn’t self-executing. Federal regulators (DOL/HHS/Treasury) and state insurance departments audit plans—especially NQTLs. Plans must produce comparative analyses showing their prior auth, step therapy, and network rules are no more stringent for SUD/MH than for medical/surgical care. Weak documentation or clear asymmetries can trigger corrective action.
Regulators set time-and-distance and appointment wait-time standards and require access to essential community providers. But if reimbursement is too low, networks thin out and patients get pushed out-of-network—a de facto parity failure. Raising rates, tightening adequacy standards, and auditing directories are the main tools here.
Coverage parity for tele-behavioral visits and permanent post-pandemic flexibilities (e.g., audio-only when appropriate) extend reach to rural and underserved areas. Integration and reimbursement for 988 call centers, mobile crisis teams, and crisis stabilization units determine whether people in acute need get rapid, non-carceral care.
Seemingly small administrative choices have outsized clinical effects: formulary tiering, prior-auth bans/limits for buprenorphine and naltrexone, whether methadone is accessible beyond opioid treatment programs, any mandatory counseling tie-ins, and refill/bridge-prescription policies. These knobs decide how quickly evidence-based medications for opioid and alcohol use disorders get into patients’ hands—and stay there.
State levers
States can pass parity laws that exceed federal baselines; expand scope-of-practice (e.g., nurse practitioners/physician assistants prescribing buprenorphine); fund and cover harm-reduction (naloxone distribution, syringe services, drug-checking); and use Medicaid rate-setting and quality metrics to strengthen networks and retention.
As major buyers, Medicaid and state employee plans can demand stronger parity compliance, broader networks, MAT-friendly UM rules, tele-behavioral parity, and equity-focused access metrics in contracts with managed-care organizations and insurers.
Why these pillars matter
Together, they determine what behavioral-health services must be covered, how hard they are to access (NQTLs, networks, costs), and where patients fall out of the access funnel. Strengthen any one pillar and you reduce leakage; align them, and you convert statutory promises into real-world treatment and recovery.
Regulation and Structure of Markets for Addictive Substances
Central to addiction policy debates is the question: How should markets for potentially addictive substances be regulated and structured? Policymakers face critical choices about balancing public health goals, consumer freedoms, and market dynamics, determining who profits, who can access these products, and under what conditions. Historically, two main strategies have shaped these markets: supply-side policies, aiming to restrict the availability or increase the price of substances, and demand-side policies, intended to reduce consumers’ desire or capacity to use these substances.
Supply-Side Policies: Controlling Availability and Price
Supply-side controls attempt to limit the availability or increase the cost of addictive substances, affecting both legal and illicit markets. “Availability” is itself latent, inferred through these market-level indicators rather than observed as a single, direct quantity. In legal markets, these policies include prescription regulations, licensing systems, production quotas, and age restrictions. For instance, the U.S. Drug Enforcement Administration (DEA) enforces strict quotas on opioid medication production, directly limiting the supply of opioids available to consumers. The logic is that making drugs scarcer or more expensive will decrease their use by increasing economic and logistical barriers to consumption (National Research Council, 1996).
In illicit markets, supply-side efforts predominantly involve interdiction—seizing drugs at borders, dismantling trafficking networks, and crop eradication. Historically, enforcement efforts during the U.S. “War on Drugs” temporarily raised prices for illicit substances like cocaine and heroin in the 1980s. However, prices largely flattened or declined in subsequent decades despite continued rigorous enforcement, demonstrating the adaptability of illicit markets and the limitations of purely supply-side approaches (Gallet, 2014).
The “Balloon Effect”
When U.S. states implemented prescription drug monitoring programs (PDMPs) to reduce opioid prescriptions, there was a notable decline in prescriptions by approximately 6%; however, heroin overdose deaths surged by over 50%, demonstrating that individuals turned to illicit markets when prescription access was restricted (University of Texas at Dallas, 2022). This phenomenon, termed the “balloon effect,” indicates that suppressing drug supply without addressing underlying demand simply shifts drug-seeking behavior rather than eliminating it entirely. We saw similar balloon effects in cannabis legalization. Overly high taxes on legal cannabis may inadvertently push users toward cheaper illicit markets, undermining legalization’s public health goals. Research suggests that excessively high taxation could paradoxically expand the black market, as price-sensitive users seek cheaper, untaxed cannabis (WHO Framework Convention on Tobacco Control [FCTC], 2022).
Potency and Product Safety Regulations
Policymakers increasingly consider potency limits and product safety standards critical to responsible substance regulation. Many U.S. states regulate the THC potency in cannabis edibles (often capped at 10mg per serving) to minimize overdose risks. Similar approaches are evident in alcohol markets, where proof limits are common to prevent excessively strong beverages. The objective is to prevent commercialization of excessively potent or
hazardous products that may heighten addiction or adverse health effects. Critics of potency caps argue they can inadvertently boost illicit markets, yet proponents view them as essential public health safeguards akin to alcohol proof limitations.
Demand-Side Policies: Reducing Consumption and Harms
Demand-side policies focus on reducing the desire and demand for addictive substances through economic and behavioral strategies. In legal markets, one of the most effective measures is taxation. High taxes on alcohol and tobacco have significantly reduced consumption rates. Nordic countries, such as Sweden and Norway, experienced notable declines in alcohol-related harm following tax increases (WHO Regional Office for Europe, 2020). Advertising restrictions are another effective demand-side tool; Norway’s ban on alcohol advertising (since 1975) markedly reduced alcohol sales and consumption, especially among youth (WHO Regional Office for Europe, 2020). Similar restrictions on tobacco and cannabis marketing aim to reduce product appeal, particularly among vulnerable groups.
In illicit markets, demand-side interventions often include educational programs, increased access to addiction treatment, and recovery services, all aiming to reduce substance demand and usage. Notably, recent U.S. drug control budgets have devoted over half their funding to demand reduction—prevention and treatment—marking a significant policy shift from the enforcement-dominant strategies of past decades (Office of National Drug Control Policy, 2023).
Regulating Advertising and Marketing
Another demand-side regulatory measure is the restriction of advertising and marketing. Such policies aim to limit the appeal and normalization of addictive substances, particularly among youth. Norway’s comprehensive ban on alcohol advertising, in place since 1975, significantly reduced alcohol consumption (WHO Regional Office for Europe, 2020). Likewise, tobacco advertising bans and plain packaging laws have successfully reduced smoking initiation globally. These insights have guided cannabis regulation in newly legalized markets in the U.S., where strict marketing controls prevent the promotion of products to youth or the exaggeration of health claims.

Summary: Regulation and Structure of Markets for Addictive Substances
Effective addiction policy requires careful management of the markets for addictive substances through balanced supply-side and demand-side policies. Although supply-side measures like prescription monitoring programs can reduce drug availability, unintended consequences, such as the “balloon effect,” highlight the importance of complementary demand-side strategies—such as taxation, advertising restrictions, and education—to sustainably reduce substance use and related harms.
Conclusion
The ABCD Study includes a wide array of policy-related variables and we provide an overview in the Appendix to this chapter. This chapter examined how public policy shapes addiction outcomes by influencing enforcement, treatment access, and the markets for addictive substances. It first traced the rise of criminalization during the War on Drugs, showing how deterrence-based strategies increased arrests and incarceration while producing enduring racial disparities and limited public health benefits. It then outlined the shift toward public health approaches, emphasizing harm reduction and treatment-based responses, and explaining how insurance design and parity enforcement can determine whether evidence-based care is accessible in practice. Finally, it analyzed how governments regulate substance markets through supply-side and demand-side policies, highlighting tradeoffs such as the balloon effect, and the role of taxation, product standards, and marketing restrictions in reducing harms.
Works Cited
Alexander, M. (2010). The New Jim Crow: Mass incarceration in the age of colorblindness. The New Press.
Becker, G. S. (1968). Crime and punishment: An economic approach. Journal of Political Economy, 76(2), 169–217.
Ennett, S. T., Tobler, N. S., Ringwalt, C., & Flewelling, R. (1994). How effective is drug abuse resistance education? A meta-analysis of Project D.A.R.E. outcome evaluations. American Journal of Public Health, 84(9), 1394–1401. https://doi.org/10.2105/AJPH.84.9.1394
Institute for Crime & Justice Policy Research. (n.d.). Highest to lowest – Prison population total. World Prison Brief. Retrieved March 11, 2025, from https://www.prisonstudies.org/highest-to-lowest/prison-population-total
Kang-Brown, J., Montagnet, C., & Heiss, J. (2021). People in Jail and Prison in 2020. Vera Institute of Justice.
Levine, H. G. (2017). Marijuana Arrest Research Project. Sociology Department, Queens College, City University of New York.
Marlatt, G. A. (1996). Harm reduction: Pragmatic strategies for managing high-risk behaviors. Guilford Press.
Nagin, D. S. (2013). Deterrence in the twenty-first century: A review of the evidence. Crime and Justice, 42, 199–263.
National Research Council. (1996). Pathways of addiction: Opportunities in drug abuse research. National Academies Press.
Pew Research Center. (2011). The effects of incarceration on crime and the cost of imprisonment.
Room, R. (2021). Government monopoly as an instrument for public health and welfare: Lessons for cannabis from experience with alcohol monopolies. International Journal of Drug Policy, 91, Article 102747.
Sawyer, W., & Wagner, P. (2025, March 11). Mass incarceration: The whole pie 2025. Prison Policy Initiative. Retrieved from https://www.prisonpolicy.org/reports/pie2025.html
Sheehan, B. E., Grucza, R. A., & Plunk, A. D. (2021). Association of racial disparity of cannabis possession arrests among adults and youths with statewide cannabis decriminalization and legalization. JAMA Health Forum, 2(10), e213435. https://doi.org/10.1001/jamahealthforum.2021.3435
The Pew Charitable Trusts. (n.d.). Medication-assisted treatment improves outcomes for patients with opioid use disorder. Retrieved from pewtrusts.org
U.S. Department of Justice. (2020). Justice Department announces global resolution of criminal and civil investigations with opioid manufacturer Purdue Pharma.
University of Texas at Dallas. (n.d.). Has prescription monitoring curbed the opioid epidemic? Retrieved from www.utdallas.edu
World Health Organization Framework Convention on Tobacco Control (FCTC). (2022). Does sin tax facilitate the illicit market? World Health Organization.
World Health Organization Regional Office for Europe. (2020). Reducing alcohol consumption the Nordic way: Alcohol monopolies, marketing bans, and higher taxation. World Health Organization.
Appendix: ABCD Policy Variables
The ABCD dataset includes a wide array of policy-related variables designed to capture state-level differences in social attitudes and drug-related policies. These variables span multiple dimensions, including measures of bias (immigration, gender, and race), state cannabis legalization categories, Medicaid expansion under the Affordable Care Act (ACA), and various state policies related to opioid overdose prevention and prescription drug monitoring. For example, the bias measures use data from sources like Project Implicit, the General Social Survey, and the American National Election Survey to quantify implicit and explicit biases at the state level. Cannabis legalization categories are derived from legal reviews and classify states according to their regulatory frameworks (e.g., recreational, medical, low THC/CBD, or no legal access). Other policy variables capture whether states have expanded Medicaid, as well as detailed dimensions of opioid-related policies such as co-prescribing naloxone laws, Good Samaritan laws, naloxone distribution laws, and prescription drug monitoring programs (PDMPs). Finally, additional variables provide context on opioid prescription dispensing rates (from CDC data) and residential history, which is essential for linking policy exposure over time.
These variables allow researchers to examine how state-level policy environments may interact with health outcomes and addiction behaviors, and they provide critical insights into the role of structural factors – such as biases and regulatory approaches – in shaping the lived experiences of individuals.
| Policy Category & ABCD Table Name (5.0 Release) | Measure Description |
|---|---|
| Immigration Bias Measures (led_l_biasimm) |
State-level measures of bias derived from data on implicit and explicit attitudes toward Latinx individuals. These measures reflect the influence of state-level immigration policies on the experience of all Latinx-identified individuals within a community. |
| Gender Bias Measures (led_l_biasgender) |
Measures based on implicit and explicit attitudes about gender, including indicators of women’s economic and political statuses and reproductive policies. Data are sourced from Project Implicit, the General Social Survey, and the American National Election Survey. |
| Race Bias Measures (led_l_biasrace) |
State-level measures of bias derived from both implicit and explicit data about race. These measures use data from surveys and projects to quantify racial bias across states. |
| Cannabis Legalization Categories by State (led_l_lawsmj) |
Categorizes state cannabis laws into four groups: Recreational, Medical, Low THC/CBD for medical conditions, and No Legal Access. This classification is based on legal reviews from sources such as NCSL and MPP, and is used to assign cannabis policy categories based on participant addresses. |
| ACA Medicaid Expansion Data (led_l_aca) |
Indicates whether a state adopted Medicaid expansion statewide under the Affordable Care Act or via a Section 1115 waiver, mapped to participants’ residential history based on the date of policy adoption. |
| OPTIC-Vetted Co-prescribing Naloxone Policy Data (led_l_rxnalox) |
Captures state policies that require physicians to co-prescribe naloxone with opioid and/or benzodiazepine prescriptions, including dimensions for both any co-prescribing policy and those that apply universally to patients. |
| OPTIC-Vetted Good Samaritan Policy Data (led_l_goodsam) |
Reflects state Good Samaritan laws providing limited immunity (civil and/or criminal) to individuals seeking help during an overdose, including protection from arrest for controlled substance possession. |
| OPTIC-Vetted Naloxone Policy Data (led_l_polnalox) |
Contains state-level data on naloxone policies, including variables for any naloxone law in effect, those that allow distribution via standing orders or protocols, and laws granting prescriptive authority to pharmacists. |
| OPTIC-Vetted PDMP Policy Data (led_l_rxmonit) |
Encompasses state legislation on Prescription Drug Monitoring Programs (PDMPs), including indicators for any PDMP law, the implementation of modern electronic PDMP systems, and mandates requiring prescribers to access PDMP databases before prescribing opioids. |
| OPTIC-Vetted Medical Marijuana Policy Data (led_l_medmj) |
Captures dimensions of state-level marijuana policies, including indicators for medical marijuana laws, recreational use, availability of legal dispensaries, and decriminalization status for possession of marijuana. |
| CDC Opioid Prescription Dispensing Data (led_l_rxopioid) |
Provides county-level measures of opioid prescriptions dispensed per 100,000 residents, using data from IQVIA Xponent. The dataset includes multiple variables corresponding to prescription rates in the year of the baseline visit and for several preceding years. |
| Residential Address Description Variables (led_l_admin) |
Contains variables related to participants’ residential stability, including the percentage of time spent at primary, secondary, or tertiary addresses and the number of years of residence at a given address, which supports the mapping of policy exposure over time. |
