
2 Measuring Addiction & Youth Substance Use
Reading Objectives:
- Define Addiction: Understand addiction as a chronic, relapsing brain disorder with distinct criteria for classification.
- Operationalize Addiction: Learn how abstract constructs like addiction are translated into measurable variables using both observed and latent indicators.
- Explore Instrumentation: Examine the survey and toxicology tools employed in the ABCD Study to measure youth substance use, emphasizing data reliability and validity.
Key Terms:
- Addiction: A chronic, relapsing disorder marked by compulsive drug seeking and use despite harmful consequences.
- Substance Use Disorder (SUD): A DSM-based classification of problematic substance use patterns, varying in severity.
- Operationalization: The process of defining how an abstract concept (e.g., addiction) is measured in observable terms.
- Observed Variable: Directly measurable data (e.g., self-reported height, income).
- Latent Variable: An unobservable construct inferred from multiple observed indicators (e.g., addiction severity).
- Instrumentation: The tools and methods used to collect data.
- Survey Instrument: A questionnaire or form used to collect data on beliefs, attitudes, or behaviors.
- Toxicology: Biological testing (e.g., saliva, urine, hair) used to verify substance use and complement self-reported survey data.
Introduction
The highly controversial film “Kids” is an enduring cultural artifact of 1990s urban skater and hip hop culture in New York City, prior to gentrification. The film is known for its unfiltered portrayal of teenage drug use, sex, rape, and violence, set against the backdrop of the HIV/AIDS crisis. Actors were cast from a city park, including a young Rosario Dawson, making the film’s depiction of youth culture feel uncomfortably real. There are many valid criticisms of the movie, including that it is an exaggeration that relies on shock-value, fails to capture community and meaning-making among youth, and does not critically engage issues of race, gender, and HIV. However, the film sparked conversations about challenges facing urban teenagers at the time, highlighting existential nihilism punctuated by normalized substance use and risk-taking. Pathways to addiction start when we are young. How has youth substance use evolved, and do we measure and assess it?

Think about your experience in high school, many of us saw plenty of substance use and experimentation among our peers and acquaintances (and even family), and even more so after high school. Such exposure can potentially alter the brain’s developmental course, affecting cognitive functions (e.g., decision-making and reasoning) and possibly leading to addiction and mental health issues. For these reasons, we will examine substance addiction concepts with the ABCD study (Volkow, Koob et al. 2018). We begin by understanding how addiction concepts are measured.
In this module, we will explore survey instruments used to assess adolescent substance use, focusing on how surveys can operationalize complex constructs and collect descriptive data. The content is organized into the following parts:
- Defining Addiction: We begin by reviewing contemporary scientific definitions of addiction, highlighting its characterization as a chronic, relapsing brain disorder and discussing the impact of substance use on behavior and brain function.
- Operationalizing Addiction: Next, we explain the process of operationalization, detailing how abstract constructs like addiction are translated into measurable variables through both observed indicators and latent constructs.
- Measurement and Instrumentation: We then examine the tools and methods used to capture addiction-related behaviors. This section covers survey instruments and provides insight into how these instruments are designed to yield reliable, valid data.
- Survey and Toxicology Instruments in ABCD – Finally, we focus on the specific instruments used in the ABCD study. We detail various survey instruments aligned with DSM-5 criteria and describe complementary toxicology assessments that enhance the accuracy of self-reported data.
Defining & Operationalizing Addiction
Defining Addiction
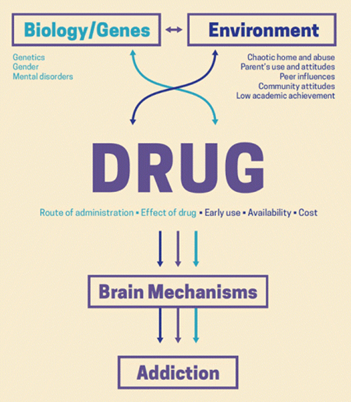
The science of addiction shows us that addiction is not a moral failure. As stated by Nora D. Volkow, head of the National Institute on Drug Abuse (NIDA), “Recent studies have shown that repeated drug use leads to long-lasting changes in the brain that undermine voluntary control” (Volkow and Li 2004). In other words, using drugs repeatedly can change the brain in ways that make it difficult for individuals to stop using drugs even if they want to. And what about the drug use before these brain changes take hold? As we will see throughout this course, our inherited personality traits and the social environments into which we are born can be strong explanations of addiction. So, what is addiction?
“Addiction is defined as a chronic, relapsing disorder characterized by compulsive drug seeking and use despite adverse consequences. It is considered a brain disorder, because it involves functional changes to brain circuits involved in reward, stress, and self-control. Those changes may last a long time after a person has stopped taking drugs” (NIDA July 2020).
In other words, drug addiction makes people feel a strong urge to seek out and use drugs even when it causes adverse events and conditions in their lives. Addiction is called a brain disorder, and often a disease, because it changes the way certain parts of the brain work, especially those parts that deal with feeling good, handling stress, and making decisions. These brain changes can last a long time, even after someone stops using drugs.
| Use… | Instead of… | Why |
|---|---|---|
| Person with a substance use disorder | Addict; User; Substance or drug abuser; Junkie | Person-first language emphasizes that substance use disorder is an illness and avoids stigmatizing labels. |
| Person with alcohol use disorder | Alcoholic; Drunk | These terms avoid implying moral failure and instead frame alcohol use disorder as a health condition. |
| Person in recovery or long-term recovery; person who previously used drugs | Former addict; Reformed addict | Neutral language avoids negative associations, punitive attitudes, and individual blame. |
Substance Addictions
Our focus in this course is substance (i.e., drug) addictions that include 10 separate classes of drugs: alcohol; caffeine; cannabis; hallucinogens; inhalants; opioids; sedatives, hypnotics, or anxiolytics; stimulants (amphetamine-type substances, cocaine, and others); tobacco; and other (or unknown) substances (Association 2013). Some of these categories are not entirely distinct from one another.
All drugs that are used in excess impact the brain’s reward system. The brain’s reward system is a group of brain structures that make you feel good when you do something enjoyable, like eating your favorite food or spending time with friends. Instead of activating the reward system through healthy activities, these substances intensely stimulate it, often causing people to neglect normal activities (Koob and Volkow 2016). The 10 drugs listed above all usually create feelings of pleasure, commonly called a “high.” However, each type of drug triggers the reward system in very different ways. For example, marijuana is psychoactive drug that can alter perception, mood, cognition, and behavior, while coffee is a stimulant that increases alertness and energy levels.
Behavioral Addictions
In addition to substances, we can also become addicted to certain behaviors, such as gambling, video games, sex, shopping, work, pornography, and more. These addictions also activate the brain’s reward system in similar ways and trigger addictive behaviors much like certain substances. However, these are not the focus of our course as we will study substance addictions.
Operationalizing Variables (Observed & Latent)
Module 1 provided a bird’s-eye view of the research process, emphasizing that to test hypotheses, we must first measure our variables. Measurement involves assigning values—quantitative or qualitative—to represent concepts we aim to study. For instance, if we want to analyze factors contributing to alcoholism, we must define what “alcoholism” (or “problematic alcohol use”) actually looks like in measurable terms. This is where operationalization comes in.
Defining Operationalization
Operationalization is the process of specifying exactly how a variable is measured. For example, to operationalize “height,” we might:
- Use a measuring tape to record exact length in inches,
- Ask participants to self-report their height in feet and inches, or
- Rank participants from shortest to tallest and categorize them (e.g., “below average,” “average,” “above average”).
Each approach yields different data, even though they measure the same concept of “height.” Similarly, in addiction research, we choose metrics that best capture whether someone meets criteria for problematic substance use.
Observed vs. Latent Variables
In the behavioral and health sciences, some variables are straightforward—like height, weight, or income. These observed variables are directly measurable, yielding raw data such as “70 inches tall” or “$40,000 annual income.”
However, more complex concepts—like addiction, motivation, or intelligence—are latent variables (constructs). They are not directly observable and must be inferred from multiple observed indicators or behaviors. For instance, addiction is often gauged by various symptoms, cravings, or consequences that a person experiences. We do not directly “see” addiction in the same way we see someone’s height; instead, we use proxies (e.g., reported frequency of use, withdrawal symptoms, tolerance) to build a composite measure of the latent construct.
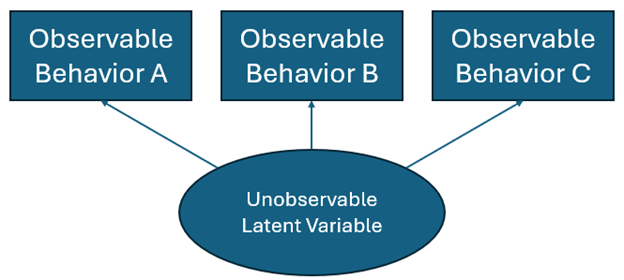
To operationalize a latent variable, researchers identify and measure several observed indicators and then combine them—often into a summary score or composite score. For example, to gauge “socioeconomic status,” we might gather data on income, education level, and occupation, then merge those into a single SES score. In the case of addiction, we may collect information on cravings, time spent recovering from substance use, and any psychosocial disruptions the substance causes.
This composite approach accounts for error or “noise,” which inevitably arises in behavioral measurement (e.g., participant mood when answering survey questions, misinterpretation of items, or variations in data collection environments). By drawing on multiple indicators, we gain a more reliable approximation of a latent construct’s true status.
Operationalizing Addiction
We had to understand the general idea of operationalizing constructs to arrive at an operational definition of addiction. The NIDA definition of addiction introduced at the top of this chapter is equivalent to a severe substance use disorder (SUD) as defined by the Diagnostic and Statistical Manual (DSM) of Mental Disorders, Fifth Edition (DSM-5, 2013; (NIDA July 2020). The DSM-5 is the American Psychiatric Association’s professional reference book on mental health and brain-related conditions, and it serves as the standard guide for clinical practice in the US.
In the DSM, a Substance Use Disorder (SUD) is diagnosed based on a pattern of behaviors related to substance use, categorized into four main groups: impaired control, social impairment, risky use, and pharmacological criteria (Association 2013). There are 11 criteria, or behavioral tendencies, that are measured across the four groups.
- Impaired Control (Criteria 1-4)
- Criterion 1: Using the substance in larger amounts or for a longer time than intended.
- Criterion 2: Persistent desire or unsuccessful efforts to cut down or control use.
- Criterion 3: Spending a lot of time obtaining, using, or recovering from the substance.
- Criterion 4: Craving or a strong desire to use the substance.
- Social Impairment (Criteria 5-7)
- Criterion 5: Recurrent substance use leading to failure to fulfill major role obligations at work, school, or home.
- Criterion 6: Continued use despite having persistent or recurrent social or interpersonal problems caused or worsened by the substance.
- Criterion 7: Giving up or reducing important social, occupational, or recreational activities because of substance use.
- Risky Use (Criteria 8-9)
- Criterion 8: Recurrent substance use in physically hazardous situations.
- Criterion 9: Continued use despite knowing it causes or worsens a physical or psychological problem.
- Pharmacological Criteria (Criteria 10-11)
- Criterion 10: Tolerance, needing more of the substance to achieve the desired effect or experiencing a reduced effect when using the same amount.
- Criterion 11: Withdrawal symptoms when not using the substance, which the person may use the substance to relieve.
Clinicians or researchers assess a patient or participant for these 11 criteria for the symptoms described. They then calculate a composite score that is an additive sum of number of criteria observed in the patient or participant. This summary score determines the severity of the SUD in the patient or participant.
Severity of the SUD is based on the number of criteria met:
- Mild: 2-3 symptoms.
- Moderate: 4-5 symptoms.
- Severe: 6 or more symptoms.
The patient or participant is characterized as in early remission if they were previously diagnosed with a SUD but they have not met any of the 11 criteria for at least 3 months but less than 12 months (except craving). If the patient or participant continues to not meet the criteria for 12 months or longer then they are deemed in sustained remission.
Instrumentation: Measuring Youth Substance Use
Instrumentation
Instrumentation involves the tools and methods used to collect data. In ABCD, these range from surveys and puzzles that assess cognitive function to biological samples (e.g., saliva) and brain scans. By ensuring accurate and consistent measurement, researchers can reliably capture the concepts being studied—particularly addiction.
Quick Start: ABCD Data Dictionary
Before working with ABCD instruments, it’s essential to know how to find and interpret variables in the Data Dictionary.
- Find the table: Use the search bar or scroll to locate the instrument’s table name (e.g., abcd_ysu01).
- Preview variables: Click the 👁 (icon) to view a table’s variables.
- Read carefully: For each variable, note:
- Label (short description)
- Level (e.g., child, parent, household)
- Type (continuous, categorical, string)
💡 Tip: The ABCD team’s full guide is excellent — see Using the ABCD Data Dictionary for advanced filtering, exporting, and linking variables across tables.
Survey Instruments
Operationalizing Variables with Survey Instruments
A survey is a questionnaire designed to capture the experiences, knowledge, beliefs, attitudes, perspectives, behaviors, environments, and conditions of participants. In self-report surveys participants complete questionnaires on their own, often used for sensitive information. In interviewer-administered surveys, a researcher asks questions and records responses, ensuring clarity and completeness.
Surveys translate broad constructs (e.g., addiction) into measurable dimensions that often combine into a summary score or composite score. For instance, researchers might ask questions about substance use frequency, cravings, and social impacts, then combine responses into a summary score representing addiction severity. Surveys also collect descriptive data (e.g., demographic details or whether a participant has tried a substance) to provide important context.
Survey Structure
Surveys can collect both qualitative with open-ended questions and quantitative data with closed-ended questions. An open-ended question allows respondents to answer in their own words, providing rich, qualitative data. For example, “Describe your first experience with alcohol.” A closed-ended question offers predefined response options, making quantitative analysis easier. For example, “In a given week, how many alcoholic beverages do you drink?” with options like “0,” “1-2,” “3-4,” “5-8,” and “8 or more.” As close-ended questions provide structured, tabular data, they are much more frequently used in health research. However, particularly with the rise of natural language processing and AI tools, new ways to quantify qualitative data are emerging.
In ABCD, we will work with three common close-ended survey question structures:
- Likert Scales: Measure attitudes, beliefs, perspectives, or behaviors on a scale. Typical Likert scales are unipolar or bipolar, unipolar scales measure the intensity of a single attribute, for example, “How frequently do you consume alcohol? Never, Rarely, Sometimes, Often, Very Often.” Bipolar scales measure the direction and intensity of two opposite attributes, for example, “I feel that drinking alcohol is harmful: Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree.” In this example, as there are five options on the bipolar scale, it is referred to as a 5-point scale. These scales are ordinal measures, meaning the distances between points are not necessarily equal.
- Binary Questions: Offer two response options, such as “Yes/No” or “True/False.” For example: “Have you ever tried smoking? Yes/No.” Binary survey questions are typically nominal measures but in some instances can be ordinal.
- Multiple-Choice Questions: Provide several response options, allowing respondents to choose one or more answers. For example, “Which substances have you tried? (Select all that apply): Alcohol, Tobacco, Cannabis, None.” These survey questions are typically measured nominally, although they can be they can sometimes be ordinal depending on how they are structured and the nature of the response options.
SUDs Survey Instruments in ABCD
ABCD uses multiple surveys aligned with DSM-5 criteria to capture various aspects of addiction in adolescents, including cravings, withdrawal, and tolerance. For example, the Rutgers Alcohol Problem Index (RAPI) measures adverse consequences of alcohol consumption with 18 items reflecting experiences such as neglecting responsibilities due to drinking. The MAPI and DAPI follow a similar structure, focusing on cannabis and other drugs, respectively. These instruments ensure a comprehensive evaluation of substance use behaviors in adolescence. Tables 2.2 and 2.3 in the Chapter Appendix includes key instruments used to assess substance use disorders and its related problems.
The ABCD study employs self-report survey instruments to assess substance use among youth participants, including alcohol, cannabis, nicotine, and various other drugs. Self-report means that the study participant is asked to share/disclose their use/consumption. The primary goal is to understand patterns of substance use initiation, frequency, quantity, and associated behaviors in adolescents.
Data Collection Procedures
Administration and Confidentiality
The substance use module is administered annually to youth participants by trained research assistants using electronic devices like iPads. All questionnaires are implemented via REDCap, a secure web application for building and managing online surveys and databases. Before beginning the survey, participants are reminded of the confidentiality of their responses to encourage honest and accurate reporting.
Gating and Survey Structure
To ensure that participants are only asked relevant questions, the survey employs a “gating” procedure. Initially, participants are asked if they have heard of specific substances, such as alcohol, cannabis, nicotine, and others. If a participant has not heard of a substance, questions related to that substance are skipped. This approach prevents introducing new substances to participants and reduces the burden of answering irrelevant questions.
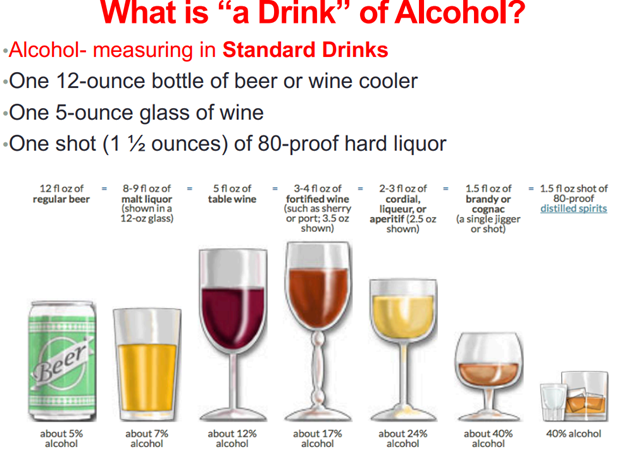
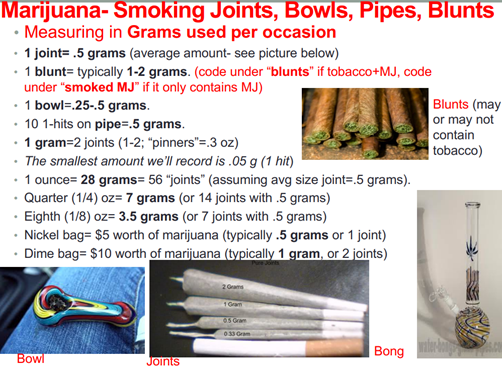
Use of Visual Aids
Visual aids play a crucial role in helping participants accurately report their substance use. For substances they acknowledge using, participants are shown images depicting standard units and modes of use. For example, standard drink sizes are illustrated to help quantify alcohol consumption, and pictures of various cannabis products assist in identifying types and typical doses. For example, below are screenshots of some of the images presented to ABCD participants during data collection.
Over Reporting Validity Check
To ensure data accuracy, the survey includes a validity check by asking about fictitious substances. If a participant endorses use of a nonexistent drug, the research assistant gently reminds them about the importance of honest reporting and allows them to amend their responses.
Substance-Specific Assessments
- Alcohol: Participants report their use of alcohol, including beer, wine, and liquor. The survey measures:
- Lifetime Use: Whether they have ever consumed alcohol.
- Age of First Use: When they first tried alcohol.
- Quantity and Frequency: Number of standard drinks consumed, frequency of use, and any binge-drinking episodes.
- Context of Use: Situations in which alcohol was consumed, including sipping during religious ceremonies.
- Cannabis and Cannabinoids: Given the complexity of cannabis products, the survey collects detailed information on:
- Types of Cannabis Products: Smoked cannabis, edibles, concentrates, synthetic cannabinoids, cannabis-infused drinks, and tinctures.
- Routes of Administration: Smoking, vaping, eating, or other methods.
- Potency and Strain: Typical strains used, THC/CBD content, and perceived potency.
- Subjective Experiences: Extent of feeling “high” and other effects.
- Source of Cannabis: Where and how participants obtain cannabis.
- Nicotine: The assessment covers various nicotine products:
- Traditional Tobacco: Cigarettes, cigars, hookah, and pipe use.
- Electronic Nicotine Delivery Systems: E-cigarettes, vape pens, and e-hookahs.
- Smokeless Tobacco: Chew, snus, and other forms.
- Nicotine Replacement Therapies: Patches, gums, nasal sprays, inhalers, and lozenges.
- Other Substances: The survey also assesses use of:
- Stimulants: Cocaine, crack cocaine, methamphetamine, prescription stimulants.
- Hallucinogens: LSD, psilocybin mushrooms, salvia divinorum.
- Club Drugs: MDMA (ecstasy, molly), ketamine, GHB.
- Opioids: Heroin, prescription opioid pain relievers used nonmedically.
- Inhalants: Substances like poppers, glue, gasoline, and nitrous oxide.
- Anabolic Steroids: Performance enhancing substances.
- Over-the-counter Medications: Cough or cold medicines containing dextromethorphan (DXM) used to get high.
For each substance, participants provide information on:
- Lifetime and Recent Use: Ever used and use in the past six months.
- Quantity and Frequency: Measured in standard units specific to each substance (e.g., grams, tablets, occasions).
- Routes of Administration: Oral ingestion, smoking, snorting, injecting, etc.
- Max Use and Typical Dosing: Highest amount used and typical dose per occasion.
- Caffeine Consumption: Given concerns about excessive caffeine use among youth, the survey assesses:
- Types of Caffeinated Beverages: Coffee, espresso, tea, soda, energy drinks.
- Typical Weekly Intake: Number of drinks per week over the past six months.
- Serving Sizes: Standardized to ensure accurate reporting.
- Maximum Daily Consumption: Largest amount consumed in one day.
Assessment of Low-Level Use
Alcohol Sipping (iSay Sip Inventory): To understand early initiation, the survey includes questions about participants’ first sipping experiences:
- Number of times sipped.
- Age at first sip.
- Context (e.g., family gatherings, religious ceremonies).
- Type of alcohol consumed.
- Whether the alcohol was offered or taken without permission.
Cannabis and Nicotine First Use: Similar assessments are conducted for cannabis and nicotine:
- First Puff or Taste: Age and context of initial use.
- Subsequent Use: Whether it led to further use.
- Subjective Effects: Feelings experienced during first use.
ABCD Substance Use Toxicology Instruments
In addition to self-report surveys, the ABCD study employs various toxicology instruments to objectively assess substance use among participants. Toxicology testing provides biological evidence of substance use, which complements self-reported data and enhances the accuracy of substance use assessments. These instruments are crucial for verifying participant reports and detecting substances that might not be disclosed.
Data Collection Procedures
Biological Samples Collected
At baseline and annual follow-up sessions, the ABCD study collects multiple types of biological samples from youth participants to screen for recent and past substance exposure. The samples include:
- Breath Samples: To detect current alcohol use.
- Saliva Samples: For recent (past 1–3 days) use of various substances.
- Hair Samples: To assess substance use over the past one to three months.
- Urine Samples: Specifically for nicotine metabolite detection and, in later follow-ups, for broader drug screening.
Administration and Confidentiality
- Trained Personnel: All samples are collected by trained research assistants following standardized protocols.
- Confidentiality: Results are coded and securely maintained to protect participant privacy.
- Participant Safety: Positive results for substances like alcohol lead to rescheduling assessments to ensure participants are not under the influence during testing.
- Informed Consent: Participants and their guardians provide consent, understanding the scope and purpose of the toxicology assessments.
Substance Detection and Analysis
- Breathalyzer Testing
- Instrument: Dräger Alcotest 5510.
- Purpose: Measures current blood alcohol content to detect recent alcohol use.
- Procedure:
- Participants blow into the mouthpiece after taking a deep breath.
- Results are displayed immediately.
- If a positive result (≥0.001 mg/L) is obtained, the test is repeated for confirmation.
- Action on Positive Result:
- Positive results at baseline are exclusionary.
- Participants showing signs of intoxication are rescheduled for their appointment.
- Saliva Drug Testing
- Instrument: Dräger DrugTest 5000.
- Substances Detected: Amphetamines, benzodiazepines, cannabis (Δ9-tetrahydrocannabinol), methamphetamine, cocaine, methadone, and MDMA.
- Procedure:
- Participants refrain from eating or drinking for 10 minutes before the test.
- A saliva sample is collected using a swab until sufficient volume is obtained.
- The sample is analyzed, and results are available within 5–8 minutes.
- Hair Analysis
- Purpose: Provides a longer detection window (up to three months) for substance use.
- Substances Analyzed:
- Alcohol metabolites (ethyl glucuronide).
- Cannabis metabolites (11-Nor-9-carboxy-THC and cannabidiol).
- Amphetamines, methamphetamine, MDMA.
- Opiates (e.g., codeine, morphine, oxycodone).
- Cocaine and its metabolites.
- Procedure:
- A small hair sample is cut from the back of the participant’s head.
- Samples are sent to a laboratory (e.g., Psychemedics) for analysis using gas chromatography-mass spectrometry (GC/MS/MS) and liquid chromatography-mass spectrometry (LC/MS/MS).
- Selection for Analysis:
- Due to budget constraints, only a subset of samples is analyzed immediately.
- Focus is on “at-risk” participants who report substance use or intent to use.
- All collected samples are stored for potential future analysis.
- Urine Testing
- Nicotine Detection:
- Instrument: NicAlert urine test system.
- Purpose: Detects cotinine, a metabolite of nicotine, to assess recent nicotine use.
- Procedure:
- Urine samples are collected from 10% of the sample and all self-reported nicotine users.
- The test indicates cotinine concentrations within 10–15 minutes.
- Drug Screening (Introduced at 4-Year Follow-Up):
- Instrument: Allere iCup testing system.
- Purpose: Detects recent use of a range of drugs.
- Procedure:
- Urine samples are collected and tested onsite.
- Positive results are followed up with a confirmatory saliva test.
Summary of ABCD Toxicology Instruments
Table 2.4 in the Appendix provides a summary of substance use toxicology instruments used in the ABCD Study.
Key Takeaways
- Understanding Addiction: Addiction is not a moral failing but a chronic, relapsing brain disorder characterized by compulsive drug seeking and use despite harmful consequences. The DSM-5 criteria help define and classify substance use disorders, providing a structured way to assess addiction severity.
- Operationalization is Critical: Operationalization transforms abstract constructs like addiction into measurable variables. This process involves specifying exactly how each variable is measured, whether through direct observed indicators or by inferring latent constructs from multiple observed behaviors.
- Differentiating Variables: Distinguishing between observed (directly measured) and latent (inferred) variables is essential. This differentiation allows researchers to build composite scores that reliably capture complex constructs such as addiction, ensuring that the measurement is both valid and consistent.
- Instrumentation Matters: A diverse range of data collection instruments, from surveys to toxicology assessments, are used to measure substance use among youth in the ABCD Study. The design of these instruments—whether through self-report questionnaires or biological tests—directly affects the accuracy and reliability of the data collected.
Works Cited
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). American Psychiatric Publishing.
Clark, L. (Director). (1995). Kids [Film]. Shining Excalibur Films.
Hagman, B. T. (2017). Diagnostic performance of the rutgers alcohol problem index (RAPI) in detecting DSM-5 alcohol use disorders among college students. J Addict Prev, 5(2), 1-7.
Koob, G. F., & Volkow, N. D. (2016). Neurobiology of addiction: A neurocircuitry analysis. The Lancet Psychiatry, 3(8), 760–773. https://doi.org/10.1016/S2215-0366(16)00104-8
Lisdahl, K. M., Sher, K. J., Conway, K. P., Gonzalez, R., Feldstein Ewing, S. W., Nixon,
S. J., Tapert, S., Bartsch, H., Goldstein, R. Z., & Heitzeg, M. (2018). Adolescent brain
cognitive development (ABCD) study: Overview of substance use assessment methods.
Developmental Cognitive Neuroscience, 32, 80–96.
https://doi.org/10.1016/j.dcn.2018.02.007
National Institute on Drug Abuse. (2020, July). Drugs, Brains, and Behavior: The Science of Addiction. Retrieved from https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction
National Institute on Drug Abuse. (2021). Words Matter: Preferred Language for Talking About Addiction. Retrieved from https://nida.nih.gov/publications
Raykov, T., & Marcoulides, G. A. (2011). Introduction to Psychometric Theory. Routledge.
Volkow, N. D., & Li, T.-K. (2004). Drug addiction: The neurobiology of behaviour gone awry. Nature Reviews Neuroscience, 5(12), 963–970. https://doi.org/10.1038/nrn1539
Volkow, N. D., Koob, G. F., Croyle, R. T., Bianchi, D. W., Gordon, J. A., Koroshetz, W. J., … Weiss, S. R. (2018). The conception of the ABCD study: From substances to neurodevelopment and mental health. Developmental Cognitive Neuroscience, 32, 4–7. https://doi.org/10.1016/j.dcn.2017.10.002
Appendix
| Instrument Name | Years of Administration & Table Name (5.0) | Instrument Description |
| Alcohol Problems (RAPI) | Annually since baseline; su_y_alc_rapi | Symptom frequency checklist of alcohol-related problems over the past 6 months. |
| Marijuana Problems (MAPI) | Annually since baseline; su_y_can_mapi | Symptom frequency checklist of marijuana-related problems over the past 6 months. |
| Drug Problems (DAPI) | Annually since baseline; su_y_dapi | Symptom frequency checklist of “other” drug-related problems over the past 6 months. |
| KSADS—Alcohol/Drug Use Disorder (Youth) | Annually since 1-year follow-up; su_y_ksads_sud | DSM-V based symptoms and diagnoses of alcohol and drug use disorders using the KSADS-COMP. |
| PATH Nicotine Dependence | Annually since baseline; su_y_nic_dep | Symptom frequency checklist of nicotine-related problems over the past 6 months. |
| KSADS—Alcohol/Drug Use Disorder (Parent) | Baseline and annually since 2-year follow-up; su_p_ksads_sud | Parent-reported DSM-V based symptoms and diagnoses of youth alcohol and drug use disorders using the KSADS-COMP. |
| Instrument Name | Years of Administration & Table Name (5.0) | Instrument Description |
| Substance Use Phone Interview (Mid-Year) | Annually since 6-month follow-up; su_y_mypi | A series of Yes/No questions about substance use over the past 6 months, administered during mid-year interviews (e.g., 6-month, 18-month follow-ups). |
| Participant Last Use Survey (Youth PLUS; Day 1/2/3/4) | Annually since baseline; su_y_plus | Measures recent over-the-counter (OTC) or prescription medications, nicotine, and caffeine use prior to neurocognitive tasks or MRI to control for withdrawal or acute effects of these substances. |
| Substance Use Interview | Annually since baseline; su_y_sui | Provides detailed data on lifetime patterns of substance use (dose, maximum dose, first use, first regular use) and past 6-month substance use patterns via Timeline Followback (TLFB). |
| Timeline Followback Interview Results | Annually since baseline; su_y_tlfb | Web-based interview method using a calendar format to obtain specific quantitative estimates of substance use over the past 6 or 12 months. |
| Participant Last Use Survey (Parent PLUS; Day 1/2/3/4) | Annually since baseline; su_p_plus | Parent-reported measures of recent OTC and prescription medications, nicotine, and caffeine use to control for withdrawal or acute effects prior to neurocognitive tasks or MRI. |
| Instrument Name | Years of Administration & Table Name (5.0) | Instrument Description |
| Alcohol Toxicology | Annually since baseline; su_y_alc_tox | Breathalyzer assessment of current alcohol use using the Dräger Alcotest. Conducted at the beginning of each testing day. Positive results are exclusionary at baseline, and participants are rescheduled if under the influence. |
| Saliva Drug Toxicology | Annually since baseline; su_y_sal_tox | Saliva testing for recent (past 1–3 days) use of substances such as amphetamines, benzodiazepines, cannabis, methamphetamine, cocaine, methadone, and MDMA using the Dräger DrugTest 5000 system. Helps detect undisclosed substance use and complements self-reported data. |
| Hair Drug Toxicology | Annually since baseline; su_y_hair_tox | Hair samples collected to detect substance use over the past one to three months. Analysis focuses on “high-risk” participants due to budget constraints. Substances analyzed include alcohol metabolites, cannabis metabolites, amphetamines, opiates, and cocaine metabolites. All samples are stored for potential future analysis. |
| Nicotine Toxicology | Annually since first follow-up; su_y_nic_tox | Urine testing for cotinine using the NicAlert system to detect recent nicotine use. Collected from 10% of the sample and all participants who self-report nicotine use. Provides semi-quantitative results indicating levels of nicotine exposure. |
| Urine Drug Toxicology | Introduced at 4-year follow-up; su_y_uri_tox | Urine testing for recent drug use using the Allere iCup testing system. Detects a broad range of substances. Positive tests are followed up with a confirmatory saliva test to ensure accuracy. |
